Download
1 / 1
10 likes | 72 Views
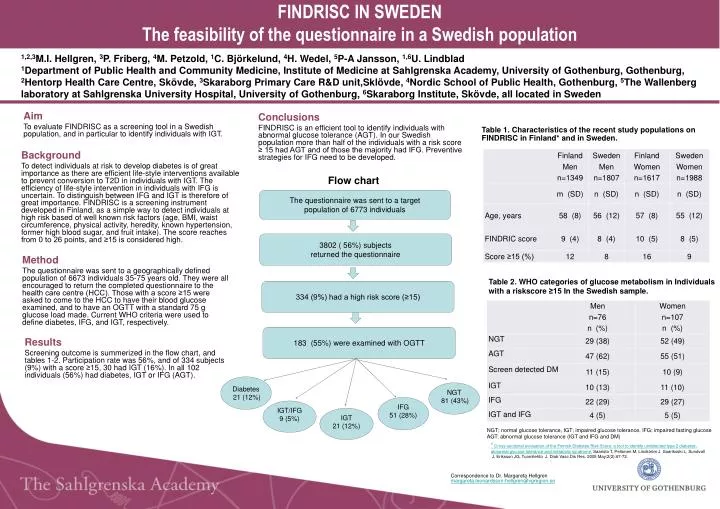
F INDRISC IN SWEDEN The feasibility of the questionnaire in a Swedish population.

E N D
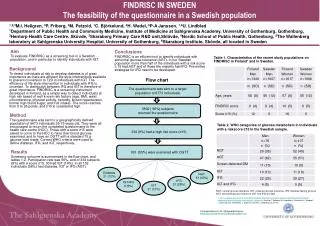
FINDRISC IN SWEDENThe feasibility of the questionnaire in a Swedish population 1,2,3M.I. Hellgren, 3P. Friberg, 4M. Petzold, 1C. Björkelund,4H. Wedel,5P-A Jansson, 1,6U. Lindblad1Department of Public Health and Community Medicine, Institute of Medicine at Sahlgrenska Academy, University of Gothenburg, Gothenburg, 2Hentorp Health Care Centre, Skövde, 3Skaraborg Primary Care R&D unit,Sklövde, 4Nordic School of Public Health, Gothenburg,5The Wallenberg laboratory at Sahlgrenska University Hospital, University of Gothenburg,6Skaraborg Institute, Skövde, all located in Sweden Aim To evaluate FINDRISC as a screening tool in a Swedish population, and in particular to identify individuals with IGT. Conclusions FINDRISC is an efficient tool to identify individuals with abnormal glucose tolerance (AGT). In our Swedish population more than half of the individuals with a risk score ≥ 15 had AGT and of those the majority had IFG. Preventive strategies for IFG need to be developed. Table 1. Characteristicsof the recent study populations on FINDRISC in Finland* and in Sweden. Background To detect individuals at risk to develop diabetes is of great importance as there are efficient life-style interventions available to prevent conversion to T2D in individuals with IGT. The efficiency of life-style intervention in individuals with IFG is uncertain. To distinguish between IFG and IGT is therefore of great importance. FINDRISC is a screening instrument developed in Finland, as a simple way to detect individuals at high risk based of well known risk factors (age, BMI, waist circumference, physical activity, heredity, known hypertension, former high blood sugar, and fruit intake). The score reaches from 0 to 26 points, and ≥15 is considered high. Flow chart The questionnairewas sent to a target population of 6773 individuals 3802 ( 56%) subjects returned the questionnaire Method The questionnaire was sent to a geographically defined population of 6673 individuals 35-75 years old. They were all encouraged to return the completed questionnaire to the health care centre (HCC). Those with a score ≥15 were asked to come to the HCC to have their blood glucose examined, and to have an OGTT with a standard 75 g glucose load made. Current WHO criteria were used to define diabetes, IFG, and IGT, respectively. Table 2. WHO categories of glucose metabolism in Individuals with a riskscore≥15 In the Swedish sample. 334 (9%) had a high risk score (≥15) 183 (55%) wereexamined with OGTT Results Screening outcome is summerized in the flow chart, and tables 1-2. Participation rate was 56%, and of 334 subjects (9%) with a score ≥15, 30 had IGT (16%). In all 102 individuals (56%) had diabetes, IGT or IFG (AGT). Diabetes 21 (12%) NGT 81 (43%) IFG 51 (28%) IGT/IFG 9 (5%) IGT 21 (12%) NGT; normal glucose tolerance, IGT; impaired glucose tolerance, IFG; impaired fasting glucose AGT: abnormal glucose tolerance (IGT and IFG and DM) * Cross-sectional evaluation of the Finnish Diabetes Risk Score: a tool to identify undetected type 2 diabetes, abnormal glucose tolerance and metabolic syndrome. Saaristo T, Peltonen M, Lindström J, Saarikoski L, Sundvall J, Eriksson JG, Tuomilehto J. DiabVasc Dis Res. 2005 May;2(2):67-72. Correspondence to Dr. Margareta Hellgren margareta.leonardsson-hellgren@vgregion.se