Download
1 / 32
350 likes | 563 Views
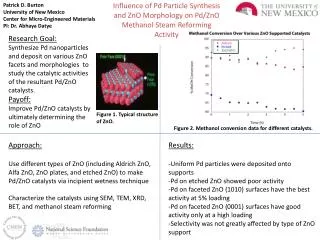
The Influence of Age and Disease on PK and PD. Matthew Walters. Influence of Disease on PK/PD. Influence of age Influence of disease: Impaired renal function Impaired hepatic function Congestive cardiac failure Gastrointestinal disease Thyroid disease. Influence of Age: Pharmacokinetics.

E N D
The Influence of Age and Disease on PK and PD Matthew Walters
Influence of Disease on PK/PD • Influence of age • Influence of disease: • Impaired renal function • Impaired hepatic function • Congestive cardiac failure • Gastrointestinal disease • Thyroid disease
Influence of Age:Pharmacokinetics • Decrease in total body water (due to decrease in muscle mass) and increase in total body fat affects volume of distribution • Water soluble drugs: lithium, aminoglycosides, alcohol, digoxin • Serum levels may go up due to decreased volume of distribution • Fat soluble: diazepam, thiopental, trazadone • Half life increased with increase in body fat
Influence of Age:Pharmacokinetics • Absorption: Not highly impacted by aging • Variable changes in first pass metabolism due to variable decline in hepatic blood flow (elders may have less first pass effect than younger people, but extremely difficult to predict)
Influence of Age: the Liver • Acetylation and conjugation do not change appreciably with age • Oxidative metabolism through cytochrome P450 system does decrease with aging, resulting in a decresed clearance of drugs • Hepatic blood flow extremely variable
Influence of Age:Excretion and Elimination • GFR generally declines with aging, but is extremely variable • 30% have little change • 30% have moderate decrease • 30% have severe decrease • Serum creatinine is an unreliable marker • If accuracy needed, do Cr Cl
The Cockroft and Gault Equation • Cr Cl = 140-age(yrs) X wt (kg) X .85 for women • Cr (mg/100ml)X72 • May overestimate Cr Cl, especially in frail elders • Useful equation, but must be aware of its limitations
Influence of Age:Pharmacodynamics • Some effects are increased • Alcohol causes increase is drowsiness and lateral sway in older people than younger people at same serum levels • Fentanyl, diazepam, morphine, theophylline • Some effects are decreased • Diminished HR response to isoproterenol and beta -blockers
Undertreatment of the Elderly • CAD • Beta blockers • ASA • Anticoagulation in AF • HTN, especially systolic HTN • Pain • Particular fear of narcotics in the elderly
Adverse Drug Reactions in the Elderly • About 15% of hospitalizations in the elderly are related to adverse drug reactions • The more medications a person is on, the higher the risk of drug-drug interactions or adverse drug reactions • The more medications a person is on, the higher the risk of non-adherence
Drug-drug Interactions • Common cause of ADEs in elderly • Almost countless – good role for pharmacist and computer or on-line programs • Some common examples • Statins and erythromycin and other antibiotics • TCAs and clonidine or type 1Anti-arrythmics • Warfarin and multiple drugs • ACE inhibitors increase hypoglycemic effect of sulfonylureas
Drug-disease Interactions • Patient with PD have increased risk of drug induced confusion • NSAIA (and COX-2’s) s can exacerbate CHF • Urinary retention in BPH patients on decongestants or anticholinergics • Constipation worsened by calcium, ahticholinergics, calcium channel blockers • Neuroleptics and quinolones lower seizure thresholds
The “Prescribing Cascade” • Common cause of polypharmacy in elderly • Some common examples • NSAIA ->HTN->antihypertensive therapy • Metoclopromide ->parkinsonism ->Sinemet • Dihydropyridine -> edema ->furosemide • NSAIA ->H2 blocker ->delirium ->haldol • HCTZ ->gout->NSAIA ->2nd antihypertensive • Sudafed ->urinary retention ->alpha blocker • Antipsychotic ->akithesia ->more meds
Renal Disease • Pharmacokinetics: • Decreased elimination • Decreased protein binding • Decreased hepatic metabolism • Pharmacodynamics: • Altered sensitivity to drug effect • Adverse effects
Decreased Elimination • Aminoglycosides • Lithium • Digoxin • Methotrexate • Penicillins • Which drugs? • Plasma concentration? • Time to steady state? • Effect on:
Decreased Elimination • Determination of renal function • Alteration of dosing schedule • Monitoring drug concentrations
Protein Binding • Renal failure leads to acid retention • “Acidic” drugs less bound to albumin: • Conformational change in albumin • Less ionised drug to bind • Increased free (active) drug in plasma • Binding of basic drugs unchanged
Protein Binding • Usually of little clinical relevance, but… • Phenytoin (acidic) • Less bound drug (more free drug) • Target concentration lower in renal failure • Effect of HD? • Effect of transplantation?
Hepatic Metabolism in Renal Failure • Hepatic metabolism of some drugs is slower in renal failure • ? Endogenous inhibitor in uraemic plasma • Normalised by HD
Pharmacodynamics in Renal Failure • Increased sensitivity to sedatives • ? BBB permeability
Other Considerations • Nephrotoxins • Fluid retention • Increasing uraemia • Electrolyte disturbances Amphoteracin, gentamicin NSAIDS Tetracyclines Amiloride, digoxin
Hepatic Impairment • Pharmacokinetics • First pass metabolism • Activation of prodrugs • Decreased protein binding • Decreased elimination • Pharmacodynamics • Altered drug effect
First Pass Metabolism • Profound changes in bioavailability: • Chlormethiazole (1000% increase) • Verapamil (140% increase) • Paracetamol (50% increase) • First pass activation reduced: • Enalapril, perindopril etc
High and Low Extraction Drugs • High extraction • Metabolised at high rate by liver • Rate varies with delivery • Affected by changes in blood flow • Morphine, verapamil, lignocaine
High and Low Extraction Drugs • Low extraction: • Metabolised at low rate by liver • Independent of blood flow • Sensitive to changes in liver enzyme activity • Chloramphenicol, theophylline
Effect on PK • Difficult to predict • Many factors involved • No simple test (cf renal impairment) • Start with low dose • TDM
Effect on PD • Sensitivity to sedatives • Sensitivity to oral anticoagulants • Precipitation of encephalopathy • Fluid retention • Hepatorenal syndrome
Congestive Cardiac Failure Mucosal oedema Blood flow • Absorption • Altered V of D • Hepatic elimination • Renal elimination ECF (oedema) Tissue perfusion Perfusion Hypoxia Congestion Perfusion Tubular reabsorption
Gastrointestinal Disease • Achlorhydria • Coeliac disease • Crohn’s More ionised acidic drug in stomach Absorption of aspirin Variable effects Gut SA Gut permeability Variable effects Gut wall thickened Altered bacterial flora Gut SA
Thyroid Disease • Digoxin • Increased sensitivity in hypothyroidism • Decreased sensitivity in hyperthyroidism • Lithium • May precipitate hypothyroidism • Check TFT’s regularly