Download
1 / 42
420 likes | 673 Views
Critical appraised topic. Binax NOW Streptococcus pneumoniae urine antigentest . Michaël Boudewijns, GSO klinische biologie. Indeling (1). Klinisch – diagnostisch scenario Vraagstelling Critical appraisal Technische performantie Klinische performantie Impact therapie en prognose

E N D
Critical appraised topic Binax NOW Streptococcus pneumoniae urine antigentest Michaël Boudewijns, GSO klinische biologie
Indeling (1) • Klinisch – diagnostisch scenario • Vraagstelling • Critical appraisal • Technische performantie • Klinische performantie • Impact therapie en prognose • Kosteneffectiviteit • Besluit
Klinisch – diagnostisch scenario (1) • Belang SRPN infecties en CAP • Etiologisch onderzoek • Microbiologisch onderzoek • “gouden standaard” • routinetesten • sneltesten
Klinisch – diagnostisch scenario (2) • S. pneumoniae (SRPN) = frequentste oorzaak community-acquired pneumonia (CAP), bacteriële meningitis, sinusitis, otitis media • CAP = frequentste ernstige aandoening met S. pneumoniae als belangrijkste verwekker
Klinisch – diagnostisch scenario (3) • CAP - jaarlijkse incidentie: 5 à 11 / 1000 volw. - hospitalisatie: 22% à 42% (5 à 10% ICU) - mortaliteit: 4% à 14% - frequentste verwekker = SRPN: * Europa: 19,4% (21,8% ICU) * risicofactoren: leeftijd, immuunglobuline deficiënties, chronische ziekte (o.a.COPD), crowding
Klinisch – diagnostisch scenario (4) • Etiologisch onderzoek • kliniek = onbetrouwbaar • microbiologisch onderzoek: rationale: • optimalisatie therapie • vernauwen spectrum • selectiedruk en resistentievorming • nevenwerkingen • epidemiologische redenen • Volksgezondheid • monitoren kiemen - resistentie
Klinisch – diagnostisch scenario (5) • Etiologisch onderzoek • microbiologisch onderzoek: • beperkingen: • lage opbrengst • 25 à 60% geen etiologie • invloed AB-gebruik • weing impact op initiële, empirische therapie • geen prospectieve studies • impact prognose • impact kosten
Klinisch – diagnostisch scenario (6) • Microbiologisch onderzoek • “gouden standaard” = cultuur geïnfecteerd longweefsel • vereist invasieve procedures • richtlijnen: • niet routinematig • evt ernstige CAP / geen respons R\
Klinisch – diagnostisch scenario (7) • Microbiologisch onderzoek • routinematig mogelijk: • Hemocultuur • Cultuur andere steriele vochten (pleuravocht) • Gramkleuring – cultuur sputum • Serologie • Moleculaire biologie • Antigendetectie • richtlijnen verschillen in aanbevelingen
Klinisch – diagnostisch scenario (8) • Microbiologisch onderzoek • cultuur steriele vochten: • zeer hoge specificiteit • lage sensitiviteit • SRPN = frequentste oorzaak bacteriëmische CAP • tot 60% van geïsoleerde kiemen • SRPN bacteriëmie: sensitiviteit max. 25% - aanbevolen door alle richtlijnen
Klinisch – diagnostisch scenario (9) • Microbiologisch onderzoek • Gramkleuring – cultuur sputum: • = controversieel • meta-analyse Gramkleuring: • onmogelijk 1 cijfer sens./ spec. • belang lokale testkarakteristieken • beperkingen: • frequent geen adequaat staal • contaminatie flora BLW • geen eenduidige interpretatiecriteria • belang knowhow laboratorium
Klinisch – diagnostisch scenario (10) • Microbiologisch onderzoek • Gramkleuring – cultuur sputum: • controverse ~ verschillende aanbevelingen: • ATS • uitzonderlijk (resistentie of ongewone kiem) • alle kiemen rapporteren • evtl verbreden therapie • IDSA • alle gehospitaliseerde patiënten • predominantie SRPN • vernauwen therapie
Klinisch – diagnostisch scenario (11) • Microbiologisch onderzoek • serologie: niet aanbevolen • PCR: = research tool • antigendetectie: • kapsel of celwand polysachariden • CIE, LA, IEA • beperkte sens./spec. + hoge kost • IDSA en BTS: enkel geselecteerde pat.
Klinisch – diagnostisch scenario (12) • Microbiologisch onderzoek • Sneltesten: = voorkeur impact initiële R\ ATS: “diagnostiek mag opstarten R\ niet vertragen neg. prognose” • Welke? • Gramkleuring sputum • PCR sputum, bloed, … • antigentest sputum, urine
Klinisch – diagnostisch scenario (13) • Microbiologisch onderzoek • Sneltesten: => in 1999 (FDA): nieuwe antigentest = ‘Binax NOW S. pneumoniae urine antigentest’
Indeling (2) • Klinisch – diagnostisch scenario • Vraagstelling • Critical appraisal • Technische performantie • Klinische performantie • Impact therapie en prognose • Kosteneffectiviteit • Besluit
Vraagstelling “ Is er een plaats voor de Binax NOW S. pneumoniae urine antigen sneltest in de etiologische diagnostiek van pneumokokken infecties, in het bijzonder van CAP?”
Indeling (3) • Klinisch – diagnostisch scenario • Vraagstelling • Critical appraisal • Technische performantie • Klinische performantie • Impact therapie en prognose • Kosteneffectiviteit • Besluit
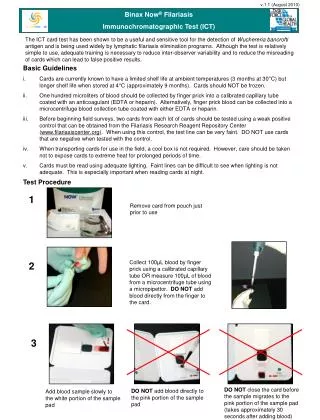
Critical appraisal: Technische performantie (1) • Principe: = immuunchromatografische test - detecteert C-polysacharide celwand SRPN - urine of CSV - snel (+/- 15 min.) - eenvoudig uitvoering interpretatie
Critical appraisal: Technische performantie (6) • enkel gegevens fabrikant • modificaties in protocol: - concentreren urine - aflezen na 5 – 60 min. - als neg. aflezen zwak pos. lijn => bemoeilijkt vergelijking studies
Indeling (4) • Klinisch – diagnostisch scenario • Vraagstelling • Critical appraisal • Technische performantie • Klinische performantie • Impact therapie en prognose • Kosteneffectiviteit • Besluit
Critical appraisal: klinische performantie (1) • Potentieel verstorende factoren: • kolonisatie BLW (nasofarynx) • voorafgaandelijk AB-gebruik • duur antigenexcretie => quid effect?
Critical appraisal: klinische performantie (2) • Kolonisatie • kinderen: • 4 prospectieve studies • jonge kinderen (< 3 j.) • gezond of diarree/dermatitis • geen recent AB of BWL-inf • prevalentie kolonisatie: 34% – 87% • pos. test: • 22% - 67% (gemid. 40,5%) dragers • 3% - 21% (gemid. 15,5%) niet-dragers = onvoldoende specifiek (bias?) Quid pos’e niet-dragers?
Critical appraisal: klinische performantie (3) • kolonisatie: • kinderen: • Belgische situatie: • 2 epidemiologische studies: • prevalentie kolonisatie: 21% (0% - 76%) en 63% => conclusie = toepassing • volwassenen: • o.a. COPD • geen goede prospectieve studies => ?
Critical appraisal: klinische performantie (4) • AB-gebruik: • slechts 1 prospectieve studie (Smith et al.): • 45 pat. SRPN CAP én pos. test • hertest op dag 3 (86% pos.) en 7 (73% pos.) => onvoldoende data voor bewijs geen effect • duur excretie: • 2 studies pat. gevolgd na genezing • 48% - 69,5% pos. na 4 – 6 wk. => suggereren persisteren
Critical appraisal: klinische performantie (5) • klinische evaluatiestudies: • bacteriëmie: 3 studies • otitis media: 2 studies • CAP: • kinderen: 2 studies • volwassenen: 10 studies • meningitis: 3 studies => meeste data CAP bij volwassenen
Critical appraisal: klinische performantie (6) • bacteriëmie: • kleine, case-control studies ( 2 retrospectief) • controlegroep: +/- inf. • sens. 82% - 95,8% • spec. 93% - 97,2% • pos. predictieve waarde (PPV): 58,8% - 96,7% • neg. predictieve waarde (NPV): 84,4% - 98,5% • suggereren een goede performantie doch, bevestigen in realistische klinische setting • otitis media: • 1 kleine, prospectieve studie (Faden et al) => suggereert probleem specificiteit (kolonisatie)
Critical appraisal: klinische performantie (7) • meningitis: • 1 grote, prospectieve studie (Samra et al) • sens. urine / CSV: 57,1% / 95,5% • spec. urine / CSV: 86,3% / 100% • PPV urine / CSV: 17,6% / 100% • NPV urine / CSV: 97,9% / 99% • suggereert goede performantie op CSV Doch vraagt bevestiging • CAP bij kinderen: • 1 goede, doch kleine, prospectieve studie (Dowell et al) => suggereert probleem specificiteit (kolonisatie)
Critical appraisal: klinische performantie (8) • CAP bij volwassenen:
Critical appraisal: klinische performantie (9) • CAP bij volwassenen: • vergelijking studies = moeilijk: • modificaties protocol antigentest • ‘gouden standaard’ • inclusiecriteria • nut modificaties (concentreren) = onduidelijk
Critical appraisal: klinische performantie (10) • CAP bij volwassenen: • sensitiviteit = beter dan elk v.d. klassieke onderzoeken afzonderlijk • specificiteit = redelijk, doch prevalentie resulteert in lage PPV quid onderschatting prevalentie?
Critical appraisal: klinische performantie (11) • CAP bij volwassenen: • richtlijnen: • IDSA: • aanvaardbare test ter aanvulling klassieke testen • hoge specificiteit => vernauwen therapie • BTS: • enkel aanbevolen bij ernstige CAP
Indeling (5) • Klinisch – diagnostisch scenario • Vraagstelling • Critical appraisal • Technische performantie • Klinische performantie • Impact therapie en prognose • Kosteneffectiviteit • Besluit
Critical appraisal: impact therapie en prognose • antigentest: geen studies • algemeen: geen prospectieve studies over effect etiologische diagnose van pneumokokken infecties op therapie en prognose
Indeling (6) • Klinisch – diagnostisch scenario • Vraagstelling • Critical appraisal • Technische performantie • Klinische performantie • Impact therapie en prognose • Kosteneffectiviteit • Besluit
Critical appraisal: kosteneffectiviteit • nadeel antigentest: • hoge kostprijs (140 € / 12 test) • Oosterheert et al: • pos. test => AB vernauwen => kostenbesparing? • algoritme kost AB en diagnostiek • potentiële reductie bij streamlinen AB • proportie pos. test • prijsverschil streamlinen AB • Nederlandse praktijk: geen besparing => kosteneffectiviteit: niet bewezen
Indeling (7) • Klinisch – diagnostisch scenario • Vraagstelling • Critical appraisal • Technische performantie • Klinische performantie • Impact therapie en prognose • Kosteneffectiviteit • Besluit
Besluit: • eenvoudig en snel • verstorende factoren: • kinderen: onvoldoende specifiek (kolonisatie); volwassenen (COPD) = ? • voorafgaandelijke AB = ? • persisteren 4 – 6 wk • CAP volwassenen • sensitiviteit = beter dan elk v.d. klassieke onderzoeken afzonderlijk • specificiteit = redelijk, doch prevalentie resulteert in lage PPV (36,7 – 78,5) (quid onderschatting prevalentie) • impact AB en prognose, kosteneffectiviteit =?