Download
1 / 37
370 likes | 377 Views
This article discusses the experience of Dr. Asafu-Adjaye Frimpong, a Consultant Interventional Radiologist, in interventional radiologic spinal pain management in Ghana. It covers the categories of chronic back pain, clinical presentation, evaluation, therapeutic interventions, and the efficacy and successes of these interventions. The article highlights the role of CT-guided nerve blocks, vertebroplasty, tumor ablation, percutaneous laser disc decompression, and other interventional pain management techniques in providing relief to patients with chronic back pain.

E N D
Interventional radiologic spinal pain management-A 7 year experience in Ghana DrAsafu-Adjaye Frimpong Consultant Interventional Radiologist
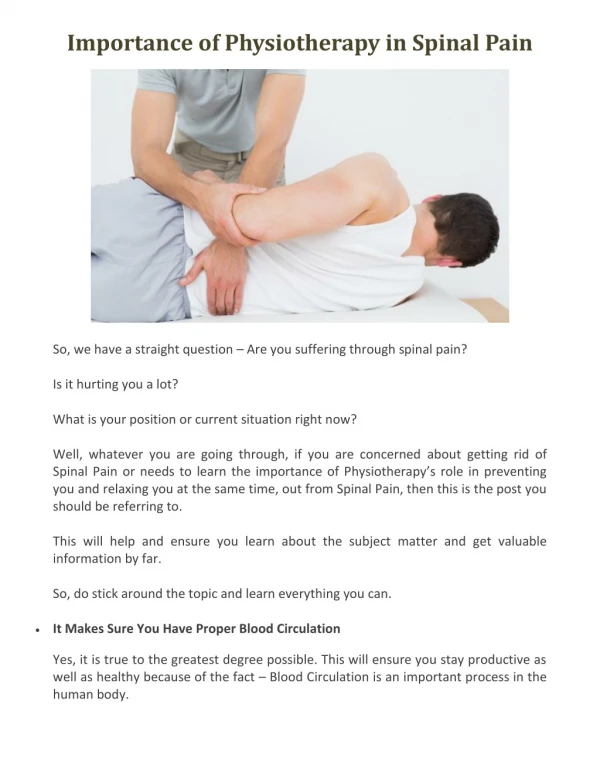
introduction • Chronic back pain is in the spectrum of neuropathic pain • Affects a significant proportion of our aged population • Affects productivity • Financial implications • Psychosocial effects
Categories of chronic backpain • Non specific back pain • Back pain associated with radiculopathy and stenosis • Back pain referred from a non spinal source • Back pain associated with another spinal cause
Mechanical from Spinal • Degenerative disk disease and facet • Herniated disk • Spinal stenosis • Traumatic fracture • Osteoporotic fracture • Congenital disease-scoliosis/kyphosis • Spondylosis
Non Mechanical Spinal • Neoplasia Metastatic carcinoma Primary vertebral tumours Multiple myeloma • Infection Septic Diskitis with abscesses Osteomyelitis • Osteochondrosis • Pagets Disease of bone • Inflammatory arthritis Ankylosisng spondylitis Reiter syndrome Psoriatic spondyloarthritis
Clinical Presentation • Focal back pain-whole spine • Radiculopathy • Claudication • Numbness and tingling • Burning sensation
Evaluation • History • Physical Examination • Labortory assessment • Imaging • Psychosocial issues
Management • Pharmacological • Non pharmacological • Interventional • Surgery
Therapeutic interventions • CT guided nerve blocks • CT guided Vertebroplasty • CT guided tumor ablation • CT guided percutaneous laser disc decompression (PLDD)
Interventional Pain management • Intrathecal drug delivery • Anesthetic nerve blocks • Neurolysis • Laser Disc Decompression • Ozone therapy
Successes with thoracic and cervical in pain control is >90% over a 2 year period • Less in lumbar region @ 70% • Recurrence of pain related to age of patient, duration and severity of disease • Generally a very safe and effective treatment for small and moderate prolapses without severe neurologic deficits • Not done for patients with weakness in limbs or atrophy. • Not very effective for treatment for numbness.
Discogenic Radiculopathy • Common in the lumbar and Cervical Region • Less common in the thoracic and Sacral regions • Access usually epidural in the lumbar region as well as selective periradicular • Cervical region usually extraforaminalperiradicular • Thoracic periradicular and transforaminal with epidural extension • 3 dose regimen of 40mg triamcinolone and 1% bupivacaine with a weekly interval
Management • Pharmacological • Non pharmacological • Interventional • Surgery
Nerve Blocks • Undertaken predominantly for pain resulting from discogenic radiculopathies • For cancer related Pain • For
Our 7 year experience in GH • Interventional pain clinic • Clinical evaluation • Imaging • Post treatment management and follow up
CT guided nerve blocks- 7 year experience • CT guided percutaneous laser disc decompression- about 3years
CT guided nerve blocks • About 4200 procedures involving about 1400 patients in 7 years were undertaken. • Categories • Age range 16-91yrs • Comprises 55% Females and 45% males
Referral Pattern • 80%-patient to patient referral • 15% from clinicians • 5% from health education and promotion
Clinical History • Low back pain with or without radiculopathy • Parathesias • Numbness and tingling • Claudication Spinalis • Pain with weakness
locations • Cervical-20% • Thoracic-< 5% • Lumbar 75% • Sacrococygeal < 1%
procedure • Planning scan • Determination of trajectory • Duration-10mins averagely • Needle placement • Confirmation of drug location and path with iodinated contrast or air • Injection of kenalog
protocol • CT guidance • 3 X procedure seperated by 1 week interval • Combination of macaine(bupivacaine) 0.25% and kenalog (triamcinolone) 40mg
Access • Transforaminal cervical • Epidural • Periradicular • Facettal • Sacroiliac
Right periradicular transforaminal T 9 block with epidural extension
Efficacy and successes • Defined as significant reduction of pain and symptoms more than 70% • Cessation of oral medication. • Short term up to 6 months • Medium term . Up to 2 years • Long term. More than 2 years
Short term- • Almost 90% success rate • Failure considered if symptoms remain the same 3 months after treatment • Seen in patients with emotional and psychosocial issues severe or absolute stenosis Grade 2+ listhesis
Medium Term • 70% • Middle Age • Moderate stenosis • History – usually up to 12 months prior to treatment
Long term- • > 50% • Younger age • Shorter duration of symptoms prior to onset of treatment • Mild to moderate prolapsed disc sizes and stenosis
complications • < 0.3% • Procedural • Medication induced
procedural • Contrast Allergy • Severe numbness • Post dural puncture headache-blood patch employed for unresolving cases • Acute back pain
Steroid Induced • Poor glycaemic control • Discoloration of the hands and sometimes skin • Menstrual irregularities • Weight gain • Increased libido and performance
limitations • Patients with severe or absolute stenosis • Poorly treated diabets • Patients with grade 2 + listhesis
Post intervention management • Review 2 weeks, 6weeks 5months • Physiotherapy • Medication • Bed rest for those presenting with acute pain
Conclusion • CT guided nerve block is a very safe, very effective therapeutic intervention for patients suffering from discogenic radiculopathy. • Limited efficacy in patients with very severe or absolute canal stenosis or grade 2+ listhesis • Complications are very minimal and usully related to general effects of steroid