Download
1 / 76
770 likes | 1.21k Views
Hallux Valgus. Hallux Valgus . Lateral deviation of the great toe and medial deviation of the first metatarsal Progressive subluxation of the first metatarsophalangeal (MTP) joint. Hallux Valgus.

E N D
Hallux Valgus Lateral deviation of the great toe and medial deviation of the first metatarsal Progressive subluxation of the first metatarsophalangeal (MTP) joint
Hallux Valgus • Static deformity due to valgus angulation of the distal articular surface of the first metatarsal or the proximal phalangeal articular surface.
Pathophysiology of Deformity • no single cause • generalized ligamentous laxity • footwear • female sex • family history • intrinsic or anatomic conditions • extrinsic causes
Pathophysiology - Extrinsic • Almost exclusively in shoe-wearing societies • Coughlin MJ, Thompson FM: The high price of high-fashion footwear, in Jackson DW (ed): Instructional Course Lectures 44. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 371-377.
Pathophysiology • Sim Fook L, Hodgson AR: A comparison of foot forms among the non-shoe and shoe-wearing Chinese population. J Bone Joint Surg 1958;40A:1058-1062 • Kato T, Watanabe S: The etiology of hallux valgus in Japan. Clin Orthop 1981;157:78-81
Pathophysiology - Intrinsic Pronation of the Hindfoot • Inman VT: Hallux valgus: A review of etiologic factors. Orthop Clin North Am 1974;5:59-66. • Hohmann G: Der hallux valgus und die ubrigen Zehenverkrummungen Ergeben. Chir Orthop 1925;18:308-376
Pathophysiology - Intrinsic • Pes planus - allows pronation of 1st MT and decreases the effect of the abductor--reported 50% incidence • Metatarsus Primus Varus - lateral deviation of MTP • Contracture of the Achilles tendon • Generalized joint laxity • Hypermobility of the first metatarsocuneiform joint • Neuromuscular disorders (including cerebral palsy and stroke).
Pathophysiology - Heredity • Hardy and Clapham noted that 63% of the 91 patients in their series had a parent who had hallux valgus • Coughlin reported that a bunion was identified in 94% of 31 mothers of children who had hallux valgus.
Anatomy The Great toe is different than lesser toes • Sesamoid mechanism • A set of intrinsic muscles that stabilize the joint and provide motor strength to the first ray
Anatomy Four groups that encircle the first MTP joint • Extensor hallucis longus and brevis • Flexor hallucis longus and brevis • Abductor • Adductor
Anatomy • Long and Short Flexors • Hood ligaments • Medial and Lateral Heads of the Flexor Hallucis Brevis inserting into the Medial and Lateral Sesamoids.
AnatomyPlantar Plate • 2 seasmoids incorporated into tendons of FHB • Plantar Plate formed by tendons of Adductor Hallucis, Abductor Hallucis, FHL and Joint Capsule
AnatomyDeforming Musculature 1. Abductor Hallucis -Inserts in the plantar aspect of the proximal phalanx -Can draw the phalanx medial and push metatarsal head lateral 2. Adductor Hallucis -2 origins -common tendon to plantar aspect of proximal phalanx and lateral aspect of plantar plate/sesamoid complex
History and Physical Examination • The primary symptom of hallux valgus is PAIN over the medial eminence. • Pressure from footwear is the most frequent cause of this discomfort. • Bursal inflammation • irritation of the skin • breakdown of the skin may be noted.
Patient EvaluationHISTORY • Must include entire patient • Family history • Symptoms • pain or just deformity • Look for presence of: • neurologic disorder • ligamentous laxity
Patient EvaluationHISTORY • Educate the patient with regard to the problem • alternatives for treatment • risks and complications when surgery is indicated • A patient's preoperative expectations play a major role in his or her postoperative satisfaction.
Patient EvaluationHISTORY • Relief of pain is frequently the major objective • Improved appearance of the foot • Ability to wear smaller or narrower shoes
Patient EvaluationHISTORY • Mann RA: Decision-making in bunion surgery, in Greene WB (ed): Instructional Course Lectures XXXIX. Park Ridge, IL, American Academy of Orthopaedic Surgeons, 1990, pp 3-13. • “while 59% of patients were able to wear their choice of shoes after repair of a hallux valgus deformity, 41% were not.”
Patient EvaluationPHYSICAL EXAM • Skin • calluses, areas of redness • Sites of pain • Motion of 1st MTP joint-increased or decreased • Mobility and structure of foot in general • Gait analysis
Patient EvaluationPHYSICAL EXAM • The patient sitting and standing • accentuated with weightbearing • Pes planus deformity • Contracture of the Achilles tendon • Magnitude of the Hallux Valgus deformity • Pronation of the great toe
Patient EvaluationPHYSICAL EXAM • Passive and active range of motion of the MTP joint is measured • Pain or crepitus, or both, with motion of the MTP joint • Metatarsocuneiform joint for hypermobility • Examiner grasps the first metatarsal with the thumb and index finger and pushes it in a plantar lateral-to-dorsomedial direction. • Mobility of more than 9 mm represents hypermobility
Patient EvaluationRadiographic Examination • Weightbearing AP • Lateral • Axial (Sesamoid)
Patient EvaluationRadiographic Examination Weightbearing AP/Lateral • Assess for bone and joint deformity • Length and shape of 1st MT • Congruent vs. Incongruent joint • Osteoarthrosis • Forefoot alignment is evaluated for metatarsus Adductus • Hindfoot is Inspected for Pes Planus or Pes Cavus.
Patient EvaluationRadiographic Examination • Measure Angles • Hallux Valgus angle • Intermetatarsal angle • Distal Metatarsal Articular Angle (DMMA) • Proximal Phalangeal Articular Angle (PPAA)
Patient EvaluationRADIOGRAPHY • Hallux Valgus Angle • Intersection of longitudinal axis of 1st MT and proximal phalanx. • Normally < 15 degrees
Patient EvaluationRADIOGRAPHY • Intermetatarsal Angle • Intersection of 1st and 2nd MT • normally < 9 degrees • increased with metatarsus primus varus
Patient EvaluationRADIOGRAPHY Distal Metatarsal Articular Angle • Defines the relationship of the distal articular surface of the 1st MT to the longitudinal axis. • Quantities the magnitude of lateral slope of articular surface.
Patient EvaluationRADIOGRAPHY • With subluxation, the articular surface deviates laterally in relationship to the 1st Metatarsal. • Usually < 6 degrees.
Patient EvaluationRADIOGRAPHY Congruency of MTP joint • Will determine appropriate surgical repair. • An intra-articular repair, or soft tissue repair in the presence of a congruent joint is at a high risk to develop postoperative stiffness or recurrence.
Patient EvaluationRADIOGRAPHY Metatarsocuneiform Joint • Key role in alignment of first ray. • Increased IM angle consistent with juvenile HV • Theorized that IM deformity or metatarsus primus varus is often the primary deformity and hallux valgus follows. • Hypermobility may predispose to recurrence.
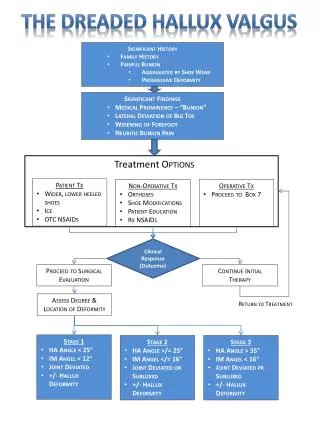
Classification Mild, Moderate, and Severe
Classification : Mild • Hallux valgus angle of less than 20° • First-second intermetatarsal angle of 11° or less. • Subluxation of the lateral sesamoid, as measured on an AP radiograph, is less than 50%.
Classification : Moderate • Hallux valgus angle of 20° to 40° • First-second intermetatarsal angle of less than 16° . • 50% to 75% Subluxation of the lateral Sesamoid.
Classification : Severe • Hallux Valgus angle of more than 40° • First-second intermetatarsal angle of 16° or more • More than 75% subluxation of the lateral sesamoid.
Treatment • Non-operative vs. Operative • All patients should be treated non-operatively first. • Important to decide whowants the treatment--parents or the patient. • Pain more important than cosmesis.
TreatmentNON-OPERATIVE Footwear Modification • Widen toe box • decrease lateral deviation of great toe • decrease inflammation and pain • Decrease heel height • prevent forward slide of the foot • Arch support • may negate effects of pes planus
TreatmentNON-OPERATIVE Contracture of the Achilles tendon • Stretching exercises • Lengthening of the Achilles tendon
TreatmentNON-OPERATIVE Grioseo, Jorge; JBJS 1992 • 56 pt. between ages of 1 mo. and 16 yr. • Treated with thermoplastic night splint and passive and active exercises until maturity. • Follow up 2-6 yr. • 50 % had improvement in HV or IM angle. • No recurrences in those that improved.
TreatmentNON-OPERATIVE Active Exercises
TreatmentSURGICAL Despite conservative measures, some patients eventually need surgical intervention.
TreatmentSURGICAL • Indications: • Persistent symptoms not cosmetic complaints • Progression of deformity • Failure of non-operative treatment • Goals: • Correct all pathologic elements and yet maintain a biomechanically functional forefoot • Usually will not result in a foot with normal appearance
TreatmentSURGICAL • The chosen surgical technique must correct all elements of the problem: • prominence of the medial eminence • increased valgus angulation of the proximal phalanx • increased first-second intermetatarsal angle • congruency of the MTP joint • subluxation of the sesamoids, • pronation of the great toe.
TreatmentSURGICAL Distal Soft-Tissue Reconstruction Silver popularized it by performing medial capsulorrhaphy, a medial exostectomy, and a lateral capsular and adductor release. McBride, who advocated removal of the lateral sesamoid and transfer of the adductor tendon to the lateral aspect of the first metatarsal head.
TreatmentSURGICAL Distal Soft-Tissue Reconstruction Medial and lateral procedures • If done in the presence of a congruent joint can create a non-congruous articulation. • Hallux Valgus angle <30 degrees • IMA < 15 degrees • High rate of recurrence if done without bony procedure • Medial and lateral procedures at the same time contraindicated.
Medial Procedures Tighten lax capsule advancement, plication or resection Abductor must not be detached Lateral Procedures Capsular release adductor longus release or transfer Division of transverse MT ligament risk NV bundle TreatmentSURGICAL