Download
1 / 23
240 likes | 446 Views
Management of Patients with NSTE ACS Latest Insights from CRUSADE A National Quality Improvement Initiative. Eric D. Peterson, MD, MPH Duke Clinical Research Institute Duke University Medical Center Durham, North Carolina. Author Disclosures: Research and speaker support from

E N D
Management of Patients with NSTE ACSLatest Insights from CRUSADE A National Quality Improvement Initiative Eric D. Peterson, MD, MPHDuke Clinical Research InstituteDuke University Medical CenterDurham, North Carolina Author Disclosures: Research and speaker support from Millennium, Schering Plough, BMS, Sanofi.
Aspirin Clopidogrel Beta Blocker Heparin (UFH or LMWH) GP IIb-IIIa Inhibitor Cath/PCI Aspirin Clopidogrel Beta Blocker ACE Inhibitor Statin/Lipid Lowering Smoking Cessation Cardiac Rehabilitation Goals for CRUSADEImprove Adherence to ACC/AHA Guidelines Improve Patient Outcomes Acute Therapy Discharge Therapy 2002 ACC/AHA Guidelines Update
CRUSADE Site Distribution Sites Who Have Submitted = 486 WA (8) ME (1) VT (1) ND (1) MT (0) MI NH (2) MN (4) NY (36) OR (5) MA (11) WI (5) SD (2) RI (1) ID (0) MI (24) WY (0) CT (8) PA (39) IA (4) NJ (10) NE (4) OH (30) DE (3) NV (3) IL (15) IN (9) WV (3) MD (13) VA (16) UT (1) CO (8) KY (8) MO (12) KS (3) DC (1) CA (36) NC (13) TN (15) SC (6) OK (8) AR (4) AZ (9) NM (2) AL (11) GA (15) MS (7) LA (8) TX (17) FL (33) AK (0) HI (1) Last updated: 1/28/05
CRUSADE GRACE VIGOUR RCT’s Representation of ElderlyCommunity vs. RCT Population % Age >75 Decade Lee, JAMA, 2001
Gender and Age: NSTE ACS % of population Patient Age
Age and Comorbid Illness % of population
Creatinine Clearance and AgeVIGOUR Trials and CRUSADE Median Creatinine Clearance* Patient Age (Yrs)
Acute Medication Use – Q3 2004(Within 1st 24 hours in patients without contraindications) 96% 100% 91% 88% 80% 55% 60% 46% 40% 20% 0% Beta Blockers Heparin (LMW + UFH) GP IIb-IIIa Inhibitors Clopidogrel ASA Q4 2004 CRUSADE data
Trends in Acute Therapy Adherence (Among Patients Without Contraindications) Quarter 1, 2002 through Quarter 4, 2004
Invasive Cardiac Procedures – Q4 2004(Among Patients Without Contraindications to Cath) 90% 82% 75% 75% 61% 60% 60% 52% 45% 45% 40% 55% 30% 30% 12% 15% 15% 0% 0% Cath Cath Cath < 48 hr Cath < 48 hr PCI PCI PCI < 48 hr PCI < 48 hr CABG CABG Q4 2004 CRUSADE Data
Trends in Invasive Procedure Use (Among Patients Without Contraindications to Cath) Quarter 1, 2002 through Quarter 4, 2004
The Train Speeds Up….Faster Cardiac Catheterization* * Among those receiving cath
The Train Speeds Up….Shrinking In-hospital ACS Care <3 Days 35% vs 47%
Discharge Medication Use – Q4 2004 (In patients without contraindications) 100% 94% 91% 88% 80% 72% 69% 60% 40% 20% 0% ASA Beta Blockers ACE- or ARB* Any Lipid- Lowering Agent# Clopidogrel *LVEF < 40%, CHF, DM, HTN# Known hyperlipidemia, TC, LDL
Trends in Discharge Therapy(Among Patients Without Contraindications) Quarter 1, 2002 through Quarter 4, 2004
Overall Adherence Trends Over Time Quarter 1, 2002 – Quarter 3, 2004 Quarter 1, 2002 through Quarter 4, 2004
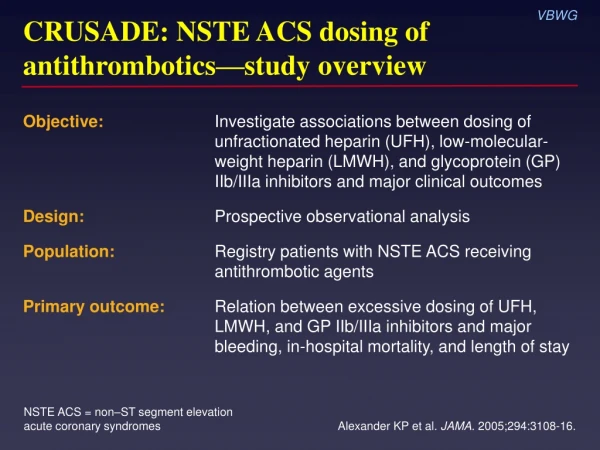
Need Right Drug but Also Right DoseExcessive Antithrombotic Dosing by Age Q1-Q2 2004 CRUSADE data:
Consequences of Excessive Dosing:RBC Transfusions by Dose Excess RBC Transfusion (%)
Does it Matter? Mortality Rates by # of Acute Guideline Recommended Therapies Received Adjusted OR: 0.72 (0.68,0.76) % In-hospital Mortality Number of Recommended Therapies * Therapies = Acute Aspirin, Acute Beta-blockers, Acute Heparin, GP IIb/IIIa inhibitors, Cardiac Catheterization <48 hours
Mortality Rates by # of Acute Guideline Recommended Therapies Received by Age Group Age Group Adj. OR* 0.71(0.67,0.75)0.79 (0.75,0.83) % In-hospital Mortality Number of Recommended Therapies * Therapies = Acute Aspirin, Acute Beta-blockers, Acute Heparin, GP IIb/IIIa inhibitors, Cardiac Catheterization <48 hours
Mortality Rates by # of Acute Guideline Recommended Therapies Received by Risk Group Risk Group % In-hospital Mortality Number of Recommended Therapies * Therapies = Acute Aspirin, Acute Beta-blockers, Acute Heparin, GP IIb/IIIa inhibitors, Cardiac Catheterization <48 hours; Based on CRUSADE Risk Score
Latest Results in NSTE ACS in US Conclusions • Crusade continues to represent ‘real world’ NST ACS • Older patients • More comorbidity • Care for NSTE ACS is improving: • Continued progress in adherence to ACC/AHA Guidelines for both acute and discharge treatments • More early cath, leading to earlier discharge • Yet opportunities for improvement persist • Largest gaps: acute GP IIb/IIIa, D/C ACE, clopidogrel • “Right dosing” to reduce adverse events • And can lead to even better patient outcomes!