Download
1 / 169
1.69k likes | 1.7k Views
Endocrine System. Thyroid Gland Adrenal Glands. Functions of endocrine system. Response to stress and injury. Growth and development. Reproduction. Homeostasis Energy metabolism. Endocrine glands. Endocrine glands are specialized cluster of cells that secrete hormones.

E N D
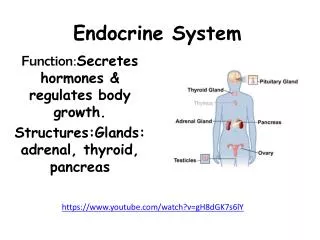
Endocrine System Thyroid Gland Adrenal Glands
Functions of endocrine system • Response to stress and injury. • Growth and development. • Reproduction. • Homeostasis • Energy metabolism.
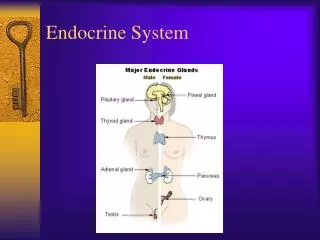
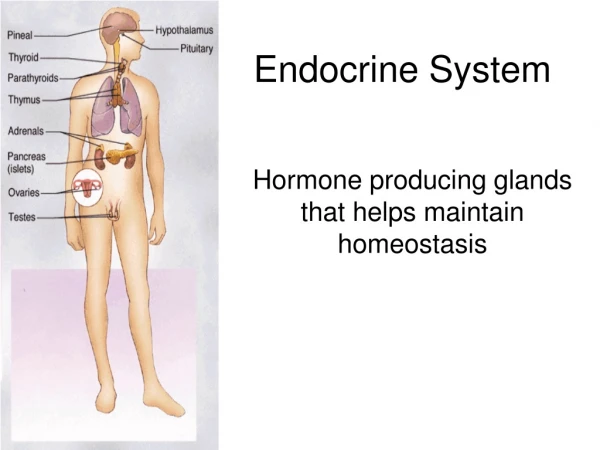
Endocrine glands • Endocrine glands are specialized cluster of cells that secrete hormones. • Secreted hormones go directly into the blood stream (ductless gland ) in respond to the nervous system stimulation. • Endocrine glands include : • The pituitary gland, thyroid gland,parathyroid glands, adrenals glands, ovaries and testes.
Hormones are chemical messengers secreted by endocrine organs and transported throughout the body where they exert their action on specific cells called target cells. Hormones do not cause reactions but rather they are regulator of tissue responses. Endocrine system
Hormones • Secreted in minimum amount in respond to need. • Either travel through the blood stream to the target organ or are secreted locally to produce an effect. • Transportation of the hormones • Bounded to plasma proteins such thyroid and steroid (they serve as a reserve for acute changes) • Some are transported free in the blood only free hormones are biological active.
Chemically hormones are of three basic types: Steroid/products of cholesterol breakdown such as glucorticoids and mineral corticoids. Monoacids analog-derivated from amino acid tyrosine (T3 and T4) Peptides either a large proteins or a chain of proteins such ACTH, TSH or ADH. Hormone structure and function
Hormones • Maintain homeostatic balance utilizing a feedback mechanism that involves other hormones, blood or chemicals,and the nervous system.
Feedback loop mechanism. • Sensors in the endocrine system detect changes in the hormonal levels. • Hormones are adjusted to maintain normal body levels.
Feedback loop mechanism. • When the sensor detect a decreased in hormone levels. They began to act to cause at increased in hormonal level. • When the hormonal levels rise above normal, the sensors cause a decreased in hormonal production.
Hormonal control • Hormones are released by your hypothalamus signals: • Anterior pituitary gland makes thyroid-stimulating hormones (TSH). • (TSH). triggers your thyroid gland to make hormones thyroxine (T4) and triiodothyronine (T3).
Can be divided into five broad categories Subnormal hormonal production, resulting from malformation, or absent of the endocrine glands, or the gland could be diseased, or destroyed or secretions are block. Hormonal excess tends to caused severe disease. Production of abnormal hormone cause by a gene mutation. Endocrine dysfunctions
Disorder of hormonal receptors. Abnormality of hormonal transport or metabolism. Disorder of the transport mainly related to lack of protein to bind the hormones. Results in increase free level of the hormone Endocrine dysfunction
Thyroid gland • A small gland shaped like a butterfly located below the larynx; it weights 15-20g. • Needs iodine to produce hormones • It produces these two hormone thyroxine and triiodothyronine.
The glands contain two types of cells Follicular cells which produce T3 and T4 Parafocicullar cells which secrete thyrocalcitonin T3=9% of the hormone secreted is in active form. T4=90% of the hormone secreted is bounded to protein as a storage form; this form is inactive until converted to T3. Thyroid hormones
Several illness Fasting Malnutrition Trauma Increased age Drugs such as propyl-thoracic (PTU) Radiologic contrast dye Dexamethasone Propranolol and amiodarone Inhibition of the conversion of T4 to T3
Laboratory thyroid tests • TSH -level (serum) • Level T4 • Level T3
Diagnostic thyroid test • RAI uptake test • A radioactive iodine RAI uptakes test measure the absorption of I -131 or I -123 by the thyroid gland. A calculated dose of radioactive iodine is given P.O or IV 24 hours later the thyroid is scan. If the uptake of iodine is increased hyperthyroidism is suspected. The side and shape of gland can be found.
Hypothyroidism • The result of decreased thyroid hormone. • Classified as primary and secondary • Age of onset is usually over 40 years • Incident higher in women 5-10:1
Pathophysiology of hypothyroidism • Lack of thyroid hormone lead to decrease in all body processes, progressing to coma • The body try to compensate by: • Peripheral vasoconstriction decrease blood flow to the extremities. • Cardiovascular= decreased blood pressure, heart rate, contractibility, cardiac output and slowed conductivity.
Pathophysiology of hypothyroidism • Interstitial accumulation of mucopolysaccharide substance (greatly increased quantities hyaluronic acid chondroitin sulfate binds with a protein to form excessive tissue gel in the interstitial spaces) • As a result, water accumulated in the interstitial spaces, which leads to nonprinting edema.
Etiology of hypothyroidism • Primary dysfunction of the thyroid accounts for 95% of all cases and be associated with the followings. • Increased dysfunction after trauma • Withdrawal of thyroid replacement therapy • Exposure to cold • Administrations of tranquilizers, barbiturates or narcotics. • Removal thyroid gland (thyroidectomy)
Etiology of hypothyroidism • Iodine deficiency • Iodine is necessary for TH synthesis and secretion. • Causes: Drugs that block TH synthesis or goitrogenic compounds in food.
Etiology of hypothyroidism • Hashimoto’s thyroid • Autoimmune disorder that destroy thyroid tissue and replace it with fibrous tissue
Radioactive iodine ablation hypothyroidism Other drugs Lithium carbonate=inhibits hormone release Dilantin (Phenytoin) decreases conversion of T4 to T3 Dopamine inhibit released TSH from the pituitary gland. Secondary dysfunction related related to pituitary dysfunction. Hypophysectomy pituitary tumor or infection Etiology of hypothyroidism
Clinical Manifestations of Hypothyroidism • Exhaustion • Depression • Dry coarse skin
Manifestations or signs and symptoms(continue) • Cold intolerance • Constipation • weight gain
Clinical manifestation of hypothyroidism • Cardiovascular=Bradycardia, hypotension , decreased contractility and cardiac output. • Neurological =Decreased LOC, lethargy, memory impairment, slow speech seizure and coma. • Most patient do not present with coma but disorientation, lethargy and confusion.
Clinical manifestation of hypothyroidism • Respiratory=hypoventilation , respiratory failure. • Gastrointestinal =weight gain with decreased appetite, constipation • Thermal : hypothermia less 35C (95F) cold intolerance.
Clinical manifestation of hypothyroidism • Edema and deposit of mucopolyssacharide substance: • skin facial= edema and enlarged tongue, • Vocal cords=hoarse • Middle ear=decreased hearing • Heart=pericardial effusion • Lungs= Pleura effusion • Bowels=paralytic ileus
Lab and diagnostic for Primary Hypothyroidism • TSH is usual increase • T3 decrease • T4 decrease
Decreased T3 uptake (measure T3 remaining after unbounded sites have been filled.) Cardiomegaly Hypoglycemia Increased cholesterol: the liver is unable to excrete cholesterol in the bile so it accumulate and leads to arteriosclerosis and leads to PVD, and CAD EKG= bradycardia and prolonged QT , low voltage Diagnostic studies
Treatment of hypothyroidism. • Pharmacological Treatments • Levothyroxine sodium (T4) • Liothyroid (T3) • Liotrix(T4 &T3)
Nursing responsibility • Give I hour before meals or 2 hours after a meal. • Watch closely patients on anticoagulants, insulin, and digitalis medications. • Assess for coronary insufficiency, CP, increased HR and dispend.
Nursing Diagnosis. • Decreased cardiac output • Alteration in bowel elimination • Alteration in Skin integrity
Assess cardiovascular system Avoid cold environment Paced activities Decreased CO r/t hypothyroidism
Decrease CO in hypothyroidism • TH deficit causes a reduction of HR and stroke volume, resulting in decreased cardiac output. • In addition it might be fluid accumulation around the pericardial sac that will further compromise the cardiac function.
Decrease CO in hypothyroidism • Assess heart rate and rhythm • Monitor cardiac function. • Fluid overload • heart failure
Hypothermia: lack of heat generation related to decreased metabolism. Monitor temperature Rewarm patient gradually and passively (plain blanket and warm room) Avoid electrical warming blanket because it can lead to vasodilatation and vascular collapse. Hypothermia