Download
1 / 12
120 likes | 179 Views
Vaginal Birth Post Cesarean Delivery: Patient Education. Diana Escobar. Vaginal Birth After Cesarean Delivery (VBAC). VBAC: successful vaginal delivery after a previous cesarean

E N D
Vaginal Birth Post Cesarean Delivery: Patient Education Diana Escobar
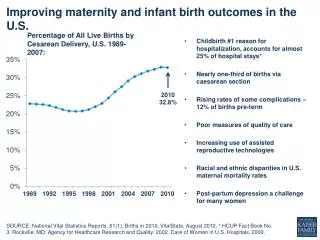
Vaginal Birth After Cesarean Delivery (VBAC) • VBAC: successful vaginal delivery after a previous cesarean • Incidence of cesarean births in the United States has increased steadily since 1996, mainly as a result of the rise in elective cesarean delivery (ECD) • The American College of Obstetricians and Gynecologists (ACOG) recognizes VBAC as a safe birthing option, & recommends cesareans should not be performed for pregnancies less than 39 weeks gestation when mothers are healthy • Women may be eligible for a trial of labor (TOL), attempt at a vaginal birth, depending on medical history, perception of pain, physician preference, comorbidities, pregnancy complications, and socioeconomic resources (Eden et al., 2013)
Research Question What is the effect of patient education (I) given during prenatal care (T), on the rate of pregnant women (P) choosing to attempt a vaginal birth after a cesarean birth (O), as compared to those who do not receive patient education (C)?
Literature Review: History • Change in policy, hospital requirements, and lack of patient education has led to a steady decline in VBACs from 26% in 1996 to 8.3% in 2007 (Eden et al., 2013) • Repeat cesarean birth rate has increased by 92% in the United States since 1996, according to McGrath, Phillips, and Vaughan (2010) • Success rates for VBACs range from 65-75%, yet only 8.5% of eligible women attempt TOL (Catling-Paull et al., 2011) • In 1999, the American College of Obstetricians and Gynecologists recommended that hospitals offering VBACs have an on call available surgical team in case of emergency (Eden et al., 2012)
Literature Review • Eden et al. (2012) reveal the ACOG hospital requirements of 1999 limited number of hospitals offering TOL because of lack of resources, liability costs, and inexperienced staff • Selecting a female obstetrician, receiving long-term care from a physician, and selecting a physician with an overall cesarean rate of less than 15% increase VBAC success (Catling-Paull et al., 2011) • Fear of a lawsuit, costs of malpractice insurance, and personal preference are predominant factors in a physician’s practice • McGrath, Phillips, &Vaughan (2010) identify patient autonomy, fear, previous experiences, education, family dynamics, economical stability, and personal choice of mothers as defining factors in VBAC attempt. • Study identified importance of evidence-based practice, patient autonomy, & personalized educational tools, as proactive interventions to increasing TOL and VBAC success. (Catling-Paull et al., 2012)
Comparative View Repeat Cesarean VBAC • Benefits • Quick postpartum recovery time • Less incidence of infection • Promotes psychosocial well-being of mothers • Decreased incidence of infant respiratory problems • Shorter hospital stay • Decreased thrombolytic events • Decreased blood loss • Complications • Increased uterine rupture risk: rate of 0.07%, especially in augmented labor • Maternal Psychosocial stress and anxiety • Cesarean for breech presentation, malpresentation, or fetal distress, spontaneous labor, & cervical dilation • Benefits • Decreased risk for uterine rupture • Less psychosocial stress on mother • Quick and more predictable birthing method • Increased Physician monitoring and prevention precautions • Complications • Longer postpartum recovery time • Increased Hemorrhage risk • Increased risk for emergency hysterectomy • Risk for infection and complications from major surgery • Lack of maternal Skin to Skin interaction Reference: (Catling-Paull et al., 2011)
Nursing and Clinical Implications • Nurse should provide unbiased education, proper education tools, and to advocate for the preferred method of delivery of their patients, especially when VBAC and ECD are equivalent options (Eden et al., 2012) • Nurse should provide decisional aids, evidence-based information, and psychosocial support (Catling-Paull et al., 2011) • Responsibility of healthcare providers in respecting and advocating for the choices of their patients (autonomy) regardless of personal preference (Catling-Paull et al., 2011) • Provision of adequate hospital and staff resources to offer women unbiased birthing options, as well as patient education during prenatal period: birthing plans, education videos, educational pamphlets, family counseling, insurance options, psychosocial support (Catling-Paull et al., 2011)
Potential Barriers • Hospital availability due to emergency resource, staff limitations, and unfriendly policy • Biased options and education based on physician choice, comfort, and fear of liability • Lack of unbiased education about VBAC: audio, video, written, and individualized educational materials • Language barriers: lack of information and education in low socio-economical groups or immigrant populations • Maternal biased view of natural birth: fear, anxiety, lack of support, psychosocial variability (Knight et al., 2013)
Ethical Considerations • Patient Autonomy: Advocating and Respecting a woman’s preferred birthing method regardless of clinician preference, comfort, or hospital or insurance preference • Justice: Clinicians are required to offer all unbiased birthing options to women when they qualify for a VBAC, and offer unbiased educational resources to inform women of options • Beneficence & Nonmaleficence: Clinicians should promote the best birthing option for women regardless of liability fears, comfort, and preference. They should refrain from performing unnecessary cesareans, and coercing patients into choosing a particular birthing option (McGrath, Phillips, &Vaughan, 2010 )
Expected Outcomes • Methods: Comparative study of pregnant women, control will only receive printed education, and experimental group will receive individualized educational plan integrating varying tools. Survey woman experience and statistical analysis of birthing method and pregnancy and fetal outcomes • Expectations: Proper unbiased education, support, and resources will increase the rate attempt TOL and the success of VBACs • Increased patient education will encourage women to attempt TOL • Interventions should lead to an overall decrease in cesarean rate & increased VBAC rate • Patient education and autonomy will increase VBAC awareness and encourage hospitals, clinicians, and insurance companies to adopt VBAC friendly policy and practice
Conclusion • Patient education, advocacy, and psychosocial support highlight the impact of the nursing role on patient autonomy • Future research should focus on increasing availability of educational materials (visual, audio, written) made available in various languages for women, during prenatal period, fetal and maternal outcomes • This should increase awareness, education, and willingness of women to attempt a VBAC
References • Eden, K.B., Denman, A., Emeis, C., McDonagh, M., Fu, R., Janik, R., Broman, A., and Guise, J. (2012). Trial of labor and vaginal delivery rates in women with a prior cesarean. Journal of Obstetric and Neonatal Nursing, 42, 583-598. doi: 10.1111/j.1552-6909.2012.01388.x • Catling-Paull, C., Johnson, R. , Ryan, C., Foureur, M.J., and Homer, C.S.E. (2011). Non-clinical interventions that increase the uptake and success of vaginal birth after cesarean section: a systematic review. Journal of Advanced Nursing. 1662-1676. doi:10.1111/j.1365-2648.2011.05662.x • Mcgrath, P., Phillips, E., Vaughan, G. (2010). Vaginal birth after caesarean risk decision-making: Australian findings on the mother’s perspective. International Journal of Nursing Practice, 16, 274-281. doi:10.1111/j.1440-172X.2010.01841.x • Knight, H., Gurol-Urganci, I., van der Meulen, J., Mahmood, T., Richmond, D., Dougall, A., & Cromwell, D. (2013). Vaginal birth after caesarean section: a cohort study investigating factors associated with its uptake and success. Bjog-An International Journal Of Obstetrics And Gynaecology, 121(2), 183-192. doi: 10.1111/1471-0528.12508