Download

1 / 210
2.17k likes | 2.58k Views
Cleft Palate &/or Velopharyngeal Inadequacy Assessment or How to Determine Nose vs. Mouth Sounds. KSHA Conference Presentation 10/01/2010. Sally Helton, MS, CCC-SLP Speech/Language Pathologist. Children’s Mercy Hospitals & Clinics Kansas City, Missouri Hearing & Speech Department

E N D
Cleft Palate &/or Velopharyngeal Inadequacy Assessmentor How to Determine Nose vs. Mouth Sounds KSHA Conference Presentation 10/01/2010
Sally Helton, MS, CCC-SLPSpeech/Language Pathologist Children’s Mercy Hospitals & Clinics Kansas City, Missouri Hearing & Speech Department 913-696-5756
Introduction • Educational Background • # Years at CMHC • # Years CMHC Cleft Palate/Craniofacial Team • # Years CMHC FFVN Team • # Years Member ACPA • Primary Job Function • Other Job Functions
Intent of Presentation • To provide information regarding diagnostic assessment for communication disorders due to cleft lip &/or palate &/or velopharyngeal inadequacy • To provide information regarding other issues that impact cleft lip &/or palate &/or velopharyngeal inadequacy • To provide information regarding importance of team approach to treatment • To provide referral criteria for more advanced assessment, perceptual &/or instrumental
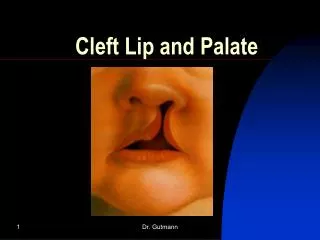
Cleft Lip • A cleft of the lip which may be: -complete or incomplete -unilateral or bilateral -extend to the nostril -extend to the alveolus
Cleft Palate • A cleft of the palate which may be: -complete or incomplete -unilateral or bilateral
Cleft Palate cont’d. -submucous -overt: observe one or more of: -bifid uvula -zona pellucida -muscular diastasis -notch in posterior border of hard palate
Cleft Palate cont’d. • Submucous cont’d. -occult (hidden)
Cleft Palate cont’d. • Variations • Incidence • Other Clefts • Classification Systems
ACPA • American Cleft Palate-Craniofacial Association
22q deletion • Deletion of genetic material from chromosome 22 • Other names: 22q11.2 deletion Shprintzen’s Syndrome Velo-Cardio-Facial Syndrome
22q deletion cont’d. • Other manifestations • Organ systems affects • Variable expression • Incidence • Significance in regard to education
Flexible Fiberoptic Video Nasopharyngoscopy (FFVN) • Invasive procedure used to evaluate the structure & function of the velopharyngeal mechanism during speech.
Velopharyngeal Mechanism • Velo: velum/soft palate • Pharyngeal: lateral & posterior pharyngeal walls • Pharynx: part of throat between esophagus & nasal cavity
Velopharyngeal Port • Port or gateway formed by action of the pharynx & velum to control the flow of air and sound through the mouth & nasal passages
Velopharyngeal Valve • Valve which closes & opens velopharyngeal port between nasopharynx & oropharynx • Formed by velum & aided by posterior & lateral pharyngeal walls • Nasopharynx: part of pharynx above soft palate & just behind nasal cavity • Oropharynx: part of pharynx below soft palate at the level of the oral cavity
Velopharyngeal Closure • Closing of nasal cavity from the oral cavity • Accomplished by using velum & pharynx & possibly adenoid tissue • Directs airflow through mouth instead of the nose
Velopharyngeal Inadequacy (VPI/A) • Generic term • Refers to any abnormal velopharyngeal function • Diagnosed perceptually (by listening)
Velopharyngeal Inadequacy cont’d. • 3 basic subtypes: -velopharyngeal insufficiency (VPI/S) -velopharyngeal incompetency (VPI/C) -velopharyngeal mislearning Subtypes CANNOT be distinguished perceptually. Subtypes are not mutually exclusive.
Velopharyngeal Insufficiency (VPI/S) • Structural defect of the palate &/or pharyngeal area
Velopharyngeal Incompetency (VPI/C) • Neurogenic impairment • Movement disorder/motor planning • Not structural
Velopharyngeal Mislearning • Functional disorder • Faulty learning of articulation patterns • Sound (phone) specific nasal air emission (s)
Relationship of VPI/A Types cont’d. • Significance of relationship: if types are not mutually exclusive, treatment will need to target all types presented by the patient
Relationship of VPI/A Types cont’d. • Significance of relationship: diagnostic assessment needs to determine types of VPI/A the patient presents diagnostic assessment should include perceptual evaluation & possible instrumental/more invasive evaluation such as FFVN
Relationship of VPI/A Types cont’d. • Instrumental diagnostic assessment with FFVN needs to be a VALID study • Use or attempted use of high pressure consonants is REQUIRED for a VALID FFVN study • If high pressure consonants are not being used/attempted, speech therapy should occur first.
History Articulation Resonance Nasal Air Emissions (NAE) Velopharyngeal Adequacy Language Voice Fluency Oral Mechanism/Oral Peripheral Examination Areas of Assessment
Tissues Gloves Flashlight Mirror Reinforcers/Toys Articulation test & score form Language test & score form Resonance/NAE protocol form (stimuli) Tape recorder (optional) Tools Needed for Assessment
Tools Needed for Assessment cont’d. • CMHC Protocol • ACPA Universal Parameters for Assessment (The Cleft Palate-Craniofacial Journal, January 2008, Volume 45, Number 1, Henningsson et.al., pg. 1-17)
Cleft: type & surgical &/or prosthetic management of Medical Speech Therapy Parents’ Concerns/Perspective School History (including learning issues) Psychological Issues Feeding/swallowing Peer Interactions Assessment-HistoryAreas to Consider
Assessment-HistoryType of Cleft/Surgeries/Prosthesis • Type of Cleft: - note type of cleft (i.e., left cleft lip & palate) • Surgeries Related to Cleft/VPI/A: - note surgeries regarding primary repair of cleft - note secondary surgeries in regard to VPI/A - note surgeries that may negatively impact VPA (i.e., tonsillectomy &/or adenoidectomy/T&A) • Prosthetic Management of Cleft/VPI: - note any prosthesis used in regard to cleft/VPI (i.e., palatal obturator, palatal lift)
Assessment-History • Medical: Pregnancy Birth Newborn period Other conditions: heart congenital anomalies Significant illnesses/diseases Audiological
Assessment-History • Speech Therapy: Enrollment: previous/ current length of enrollment # of sessions per week length per session group/ individual/combination Goals/Progress Treating SLPs name Results of Previous Evaluations
Assessment-History • Parents’ Concerns/Perspective: Start with a general question: “How do you feel (name) is doing with communication/speech?” Follow-up with specific questions regarding: understandability, articulation skills, hypernasality/NAE, voice, language skills
Assessment-History • School History: Name of School Grade Enrolled Regular Education/Special Education (or combination) Therapies Enrolled in Special Classes/Educational Help Receive Any teacher concerns regarding learning Results of recent reports/grades
Assessment-History • Psychological Issues: -Obtain results of any psychological, educational &/or IQ testing, if available.
Assessment-History • Feeding/Swallowing: -Inquire as to any history of difficulty with: sucking, chewing, swallowing -This includes both liquids & solids. - Any history of nasal regurgitation of liquids -Any issues with textures, temperatures, spiciness/blandness - Swallow studies/Oral Pharyngeal Motility (OPM) studies - History should be from birth to current age
Assessment-History • Peer Interactions: - First find out if the child has opportunities for peer interactions -Then find out if they have age-appropriate interactions with their peers or if they have difficulties
Determining Nasal Patency • Need to determine patency (airflow) of each nostril • Need to determine patency for both breathing & production of nasal sounds • If airflow is restricted or obstructed, it may mask SEVERITY &/OR INCIDENCE of resonance/NAEs
Determining Nasal Patency cont’d. • Procedure: 1. Tell the patient to blow their nose. 2. Place the mirror under both nostrils (or one at a time). 3. Tell the patient to close their mouth & breath out of their nose. 4. Keep the mirror under the nostrils. 5. Tell the patient to say /m/.
Determining Nasal Patency cont’d. • Place the mirror under both nostrils (or 1 at a time)
Determining Nasal Patency cont’d. • Tell the patient to close their mouth and breathe out of their nose.
Determining Nasal Patency cont’d. • Keep the mirror under the nostrils & tell the patient to say /m/.
Determining Nasal Patency cont’d. • Variability in Responses
Determining Nasal Patency cont’d. • Recording responses/information
Recording Nasal Patency Information Nasal Obstruction: Right Nostril Occluded Left Nostril Occluded • Inhalation/exhalation none partial complete none partial complete • Sustained /m/ (3 secs.) none partial complete none partial complete (Circle response)
Assessment-Articulation • Intent of Articulation Assessment: 1. To obtain as much information as possible regarding articulation abilities.