Download
1 / 43
430 likes | 434 Views
This lecture explores the need for an HIV vaccine, despite advancements in drug treatments and behavior-based prevention methods. It discusses the RV144 study, the history of virus vaccine technology, and the basics of adaptive immunity and immune responses to HIV. The lecture emphasizes the importance of developing a vaccine to effectively control and prevent HIV infection.

E N D
A Vaccine for HIV:31% There? African American HIV University May 19, 2014 Otto Yang, M.D. Division of Infectious Diseases, Department of Medicine, UCLA Department of Microbiology, Immunology, and Molecular Genetics, UCLA AIDS Healthcare Foundation
A Vaccine: Still the BestLong Term Solution • Drug treatments: expense, infrastructure for delivery and monitoring, treatment fatigue, toxicities, resistance • Behavior-based prevention: human nature, cultural issues • Vaccines: capacity for global impact (e.g. smallpox, polio), limited requirements for infrastructure and adherence
RV144: Mission Accomplished? • Placebo-controlled study of 16,000 people • Novel combination of two vaccines for cellular and humoral immunity • 31% protection “A job well done”?
Objectivity? PI of CHAVI ($300,000,000 consortium) PI of the $105,000,000 study ….
But where are the real numbers??? ITT: 76/7325 (1.04%) Vs 56/7347 (0.86%) PP: 50/6002 (0.83%) Vs 36/5874 (0.61%) mITT: 74/7325 (1.01%) Vs 51/7347 (0.69%)
Pre-Test Probability? Cellular Immune Component Humoral Immune Component RV144 was a test of a T-cell vaccine that failed to make T cell responses paired with an antibody vaccine that failed to make protective antibody responses So the vaccine somehow worked through a new and unintended mechanism???
How Did We Get Here? 300 Years Earlier….
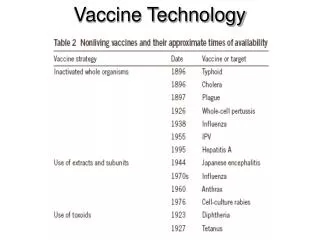
Virus Vaccine Technology: Empiricism • 1700s: Cowpox mimic of smallpox (Jenner and others) • 1950s: Killed virus (Salk) and live attenuated virus (Sabin) • 1970s: Subunit (Hilleman) • Common theme: Recapitulate infection • Protective mechanism: Who cares?
Virus Vaccine Technology: Empiricism • 1700s: Cowpox mimic of smallpox (Jenner and others) • 1950s: Killed virus (Salk) and live attenuated virus (Sabin) • 1970s: Subunit (Hilleman) • Common theme: Recapitulate infection • Protective mechanism: Who cares?
Successful Vaccines Mimic Naturally Successful Immunity Immune Response Infection MIMICKED BY VACCINE First Exposure Subsequent Exposure (LAG)
Naturally Immunity Is Unsuccessful in HIV-1 Infection Acute Infection (Flu-Like Illness) Immune Response Progression to AIDS and Death Infection Asymptomatic Phase (LAG) First Exposure Infection Subsequent Exposure Classical vaccine strategies that mimic natural immunity are therefore unlikely to work, because natural immunity fails in HIV-1 infection.
Back to the Basics…. Vaccines generate immune “memory” • B Lymphocytes- Neutralizing Antibodies • CD8+ Cytotoxic T Lymphocytes (CTLs) • CD4+ Helper T Lymphocytes (HTLs) What memory responses work against HIV?
Adaptive Immunity in a Nutshell • Adaptive immune cells (B and T lymphocytes) recognize non-self through specific receptors (BCRs and TCRs) • Receptors are generated through random genetic recombinations (about 1015 different TCRs are possible) • Self-reactive receptors are weeded out • Binding of the receptor causes a cell to mature and divide • Immune responses are generated by natural selection (clonal expansion)
Adaptive Immunity in a Nutshell Y Y Y B Y Y Y Y Y Y Y Y Y HTL VIRUS CTL
Antibodies? • The virus surface has the Env protein that is used by the virus to bind cells to infect them • Antibodies can bind Env and interfere with this process
Antibodies Don’t Control HIV-1in Infected Persons Johnston and Fauci, NEJM 2007, 356:2073-2081
CD4 binding pocket is hidden in a deep crevice Difficulties Making Neutralizing Antibodies CCR-binding region is covered until engagement with CD4 Fusion domain is covered until CCR5 engagement Envelope is heavily coated with sugars Envelope sequence is highly variable Willey et al, Trends in Microbiology 2008, 16:596-604
Neutralizing Abs NO YES NO NO NO NO NO NO NO NO NO NO NO NO YES NO NO NO NO NO NO NO YES NO NO NO NO http://www.niaid.nih.gov/about/yearinreview/advances/scientificfindings/Pages/RecentSuccessesinDevelopinganHIVVaccine.aspx
CTL Release of Cytolytic Granules and Cytokines; Signals for Apoptosis Antigen-Driven Proliferation (Clonal Expansion) Infected Cell Cellular Immunity: CD8+ Cytotoxic T Lymphocytes
CTL Recognition of Infected Cells CTL Infected Cell
HLA-I Epitope Motifs And Specificity Pathogen protein sequence Epitope Epitope Two different HLA-I molecules: Different epitopes
CTLs in HIV-1 Infection • Temporal associations with changing viremia • HLA-I associations with disease progression • GWAS studies mainly map to HLA-I • Major factor in HIV-1 sequence evolution in vivo • SIV-macaque model: CD8+ T cell depletion in vivo leads to sharply increased viremia • In vitro studies of HIV-1-specific CTL: Potent antiviral activity (cytolysis)
HIV-1-Specific CTLs Partially Control Infection Acute Infection (Flu-Like Illness) Immune Response Progression to AIDS and Death Infection Asymptomatic Phase Infection
(Weeks) (Years) Setpoint Viremia Determines Disease Progression CTLs determine setpoint, setpoint determines disease progression, thus the rationale for CTL-based vaccines to prevent disease if not prevent infection
The hope… The reality Vaccine: 24/741 Control: 21/762 VL 40k versus 37k A “Good” CTL Vaccine :STEP TrialFailure of CTLs?
Once Is Was Not Enough Vaccine: 27/1250 Placebo: 21/1244 VL similar
CTL-Based Vaccines That Mimic Nature Won’t Work • Cope with the genetic diversity of HIV-1 • Generate CTL responses at mucosal sites • Access the HLA-I pathway to elicit CTL responses against HIV-1 sequences
Mimicking HIV: Giving CTLs the Same Choices Vpu Vif Gag HIV Env Nef Tat Rev Vpr Pol Step Vaccine Gag Nef Pol HVTN505 Vaccine Gag Env Pol
The High Mutation Rate of HIV-1 Is a Huge Barrier to Immune Control • Both antibodies and CTLs work by using receptors to bind sequences in HIV • Each day, about 10 billion viruses are made in a person • Each virus has an average of 1 random mutation in its 9600 base RNA sequence • EVERY possible single or double mutation combination is made daily in vivo
Overwhelming Problem of HIV-1 Diversity From Korber, et al., British Medical Bulletin 2001: 58; 19-42.
Focus Immunity on Constrained Sequences,Rather Than Delivering Entire Proteins? OO Yang, PLoS One 2009, 4:e7388.
The Need for Speed Haase, Nature 2010, 464:217
Speed of Remembering a Vaccine O Yang, Unpublished DNA Gag/Env/Nef rAd5 Gag/Env/Nef Is There a Way to Vaccinate Constantly???