Download
1 / 17
830 likes | 5.58k Views
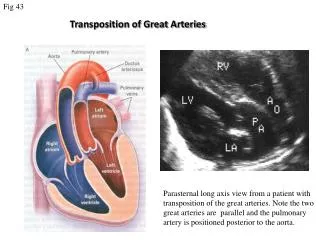
Transposition of The Great Arteries. Most common form of cyanotic congenital heart disease (5 to 7% of all congenital heart defects ) which presents in the newborn period. More common in males Babies are usually normal birth weight and size. Transposition of the Great Arteries.

E N D
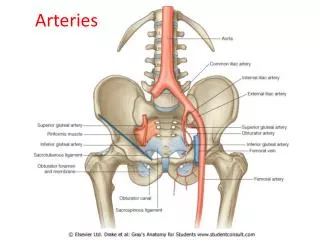
Most common form of cyanotic congenital heart disease (5 to 7% of all congenital heart defects ) which presents in the newborn period. More common in males Babies are usually normal birth weight and size. Transposition of the Great Arteries • Aorta emerges from RV 5. PDA • PA emerges from LV • VSD • ASD
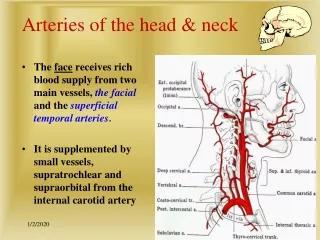
Transposition of the Great Arteries • Associated heart abnormalities: • Ventricular septal defect – the most common • Left ventricular outflow tract obstruction. • Atrial septal defect • Patent ductus arteriosus • Physical Findings: • Cyanosis, seen in lips and under fingernail beds – may not be present if baby has either an atrial septal defect and/or a patent ductus arteriosus. A ventricular septal defect is also compatible with life, but congestive heart failure will develop because of the extra blood flow going to the lungs. Sx’s consistent with CHF = poor feeding, poor weight gain, sweating, and fast or labored breathing
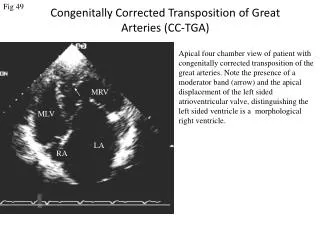
Transposition of the Great Arteries • Physical Findings: • Cyanosis will not improve with the application of oxygen – if it does, then the problem is pulmonary, not cardiac. • The second heart sound is loud and single • heart murmur, depending if there is a VSD or not • Diagnosis: • From physical findings Echo, which if not 100% definitive heart cath
Transposition of the Great Arteries • The type and timing of operation depend on the combination of defects that accompany the primary problem of TGA. • Development of early pulmonary vascular disease is also common. The changes associated with PVD can occur as early as a few weeks of life and tend to occur more frequently in babies who have ventricular septal defects in addition to TGA. Early corrective surgery minimizes the chances of development of PVD.
Transposition of the Great Arteries • Treatment: • Prostaglandin is administered until surgery can be performed to help maintain a patent ductus arteriosus • A balloon atrial septostomy can be performed during a heart cath if the cyanosis is severe – this involves passing a catheter into the right atrium and across the atrial septal defect. Once the catheter is in the left atrium a balloon is expanded and pulled back through the ASD into the right atrium enlarging the ASD, and allowing more mixing of oxygenated and deoxygentaed blood higher oxygen levels while the baby awaits surgery
Transposition of the Great Arteries • Surgical procedures: • Arterial Switch: • The aorta and pulmonary artery are divided and reconnected so that the pulmonary artery is connected to the right ventricle and supplies deoxygenated blood to the lungs. The aorta is connected to the left ventricle and supplies oxygenated blood to the body. The coronary arteries are also relocated so that they will receive oxygenated blood from the aorta. • Any septal defects are closed at the same time
Transposition of the Great Arteries • Deoxygenated blood redirected to LA • LV Lungs • Oxygenated blood from lungs redirected to RA • RV Body
Transposition of the Great Arteries • Surgical procedures: • Mustard Procedure • Used very rarely now, but most commonly done if the baby is older at diagnosis • Deoxygenated blood returning to the right atrium is redirected to the left atrium, and flows to the left ventricle where it is pumped through the pulmonary arteries to the lungs. • Oxygenated blood returning from the lungs is baffled to the right atrium, and flows to the right ventricle where it is pumped through the aorta and out to the body. • Even though the blood goes to the right location, the heart remains configured so the right ventricle (the weaker ventricle) pumps blood to the high pressure system of the aorta, and the left ventricle pumps blood to the low pressure system of the lungs.
Transposition of the Great Arteries • Deoxygenated blood redirected to LA • LV Lungs • Oxygenated blood from lungs redirected to RA • RV Body
Transposition of the Great Arteries • Surgical procedures: • Rastelli Procedure: • Performed for TGA with left ventricular outflow obstruction • The ventricular septal defect is closed in such a way that the left ventricle is connected to the aorta and the right ventricle is connected to the lungs using a conduit with a valve in it. • One end of the conduit is connected to the right ventricle where blood exits into the pulmonary artery and the other end is attached to the pulmonary artery • The conduit acts a bypass around the naturally occurring narrowing.
Transposition of the Great Arteries • Surgical procedures: • Rastelli Procedure: • This conduit will need to be replaced as the child grows. Usually this is not necessary for 3 to 5 years after the original operation if done in infancy and then 1 to 2 more times throughout the child's life.
Transposition of the Great Arteries • VSD closed with patch • Conduit
Transposition of the Great Arteries • Long-term complications of the Mustard procedure: • Systemic heart failure1,4,5,6 • Arrhythmias 1,2,3 • Venous return stasis 1 • Pulmonary edema 1 • Sudden death7 • From studies done at US and New Zealand heart centers, the overall survival rate at 10 years is ~ 80%7,8
Transposition of the Great Arteries • What happens to the pregnant pt who is status post a Mustard procedure in infancy? • Numerous studies have shown that these patients have good outcomes, overall. But they require intensive and specialized follow up.1-6 • They should be closely followed throughout pregnancy by both their cardiologist and obstetrician. • A number of these patients will develop clinical signs of right heart failure, but of these most will fully recover. 1,4,5,6 • There is a higher incidence of pre-eclampsia according to a study out of Germany 2
Transposition of the Great Arteries • What happens to the pregnant pt who is status post a Mustard procedure in infancy? • They are prone to SVT 1,2,3 • All of these patients should undergo close hemodynamic monitoring 1,4 • From all the studies reviewed, no maternal deaths occurred
Transposition of the Great Arteries • All pictures courtesy of University of Michigan Congenital Heart Center website - http://www-umchc.pdc.med.umich.edu • Rousseil MP, et al. Successful term pregnancy after Mustard operation for transposition of the great arteries. Eur J Obstet Gynecol Reprod Biol. 1995 Mar;59(1):111-3 • Reinecke H, et al. Pregnancy in patients with transposition of great vessels corrected by the Mustard procedure. Report of a case and review of reported cases. Z Kardiol. 1997 Nov;86(11):945-56 • Megerian G, et al. Pregnancy outcome following Mustard procedure fro transposition of the great arteries: a report of five cases and review of the literature. Obstet Gynecol. 1994 Apr;83(4):512-6 • Lynch-Salomon DI, et al. Pregnancy after Mustard repair for transposition of the great arteries. Obstet Gynecol. 1993 Oct;82(4 Pt 2 Suppl):676-9 • Connolly HM, et al. Pregancy among women with congenitally corrected transposition of great arteries. J Am Coll Cardiol. 1999 May;33(6):1692-5 • Therrien J, et al. Outcome of pregnancy in patients with congenitally corrected transposition of the great arteries. Am J Cardiol. 1999 Oct 1;84(7):820-4 • Wilson NJ, et al. Long-term outcome after the Mustard repair for simple transposition of the great arteries. 28-year follow-up. J Am Coll Cardiol. 1998 Sep;32(3) :758-65 • Wells WJ, et al. Intermediate outcome after Mustard and Senning procedurs: A study by Congenital Heart Surgeons Society. Semin Thorac Cardivasc Surg Pediatr Card Surg Annu. 2000;3:186-197