Download
1 / 31
310 likes | 312 Views
This case report discusses the successful treatment of a cesarean scar pregnancy, a rare form of ectopic pregnancy, through medical and surgical management. The patient achieved a live birth after the procedure.

E N D
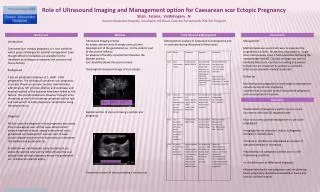
Live Birth Following Successful Treatment of Previous Cesarean ScarPregnancy: A CASE REPORT Dr. Azra Amerjee Senior Instructor Obstetrics/Gynecology Aga Khan University Hospital Karachi
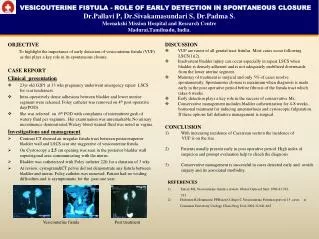
Introduction • Cesarean scar pregnancy (CSP): Rare • High index of suspicion • No universal treatment guidelines • Controversies in management • Delay: Catastrophic hemorrhage/uterine rupture • Objectives of management: Prevention of massive blood loss, preserve fertility and women’s health
Case • Twenty two years old • Gravida 3 para 1+1 • No live issue • Six weeks amenorrhea • Lower abdominal pain.
Presentation • Haemodynamically stable. • Closed cervical os • Six weeks sized uterus • No adnexal tenderness. • Serum beta-hCG level 12,040mIU/ml.
Ultrasound pelvis • 15.9 mm gestational sac, • Regular yolk sac, live fetus in previous scar line in myometrium • Endometrial cavity empty • Diminished myometrium between bladder and sac (Figure 1a, b, c,d). • No adnexal mass or fluid in Pouch of Douglas.
Management In view of: • Previous bad obstetric history • Desire to avoid surgery • Stable condition Offered and agreed for medical management with systemic Methotrexate (MTX).
Medical Management (contd) • On day 15, her BhCG level was21,303mIU/mL • USshowed GS of 9 weeks entering into endometrial cavity(Fig 2)
Surgical Management • Patient was counseled • Ultrasound guided suction evacuation was successfully performed without damage to uterus and minimal bleeding.
Outcome • Beta hCG 5 days after procedure was 412 mIU/ml • Negative after 10 days. • Normal menstrual cycles 34 days after evacuation • Conceived spontaneously after two years and recently delivered a healthy baby boy of 2800gm by Elective LSCS.
Incidence of CSP • Rare form of ectopic pregnancy • Incidence 1/1800–1/2500 of all caesarian deliveries • 6.1% of all ectopic pregnancies with at least one caesarian section. Litwicka K. CurrOpinObstetGynecol2013 Timor-Tritsch IEet al . Am J ObstetGynecol 2012 Ash A et al. BJOG 2007
Pathology • Passage of embryo through tract between uterus and old caesarean scar • Rising caesarean deliveries increase chances of pathologically adherent placenta and CSP Al-Hashmi S et. al. BMJ case reports2012 Timor-Tritsch IE et al. Am J ObstetGynecol2012
Ultrasonographic Diagnostic Criteria • Empty uterine cavity and cervix • GS anteriorly at level of internal os covering previous LSCS scar site • Increased peri-trophoblastic or peri-placental vascularity on colour Doppler • High-velocity, low-impedance flow velocity waveforms on pulsed Doppler JurkovicD et al. Ultrasound in Obstetrics and Gynecology 2003
Presentation of CSP May present between 5-16 weeks as: • Painless vaginal bleeding(39%) • Mild to moderate pain (16%) • Abdominal pain (9%) • Incidental ultrasound finding(37%) • Severe acute pain with profuse bleeding or hemodynamic instability indicates impending or ruptured CSP Al-Hashmi S et al. BMJ case reports2012 RotasMet al .ObstetGynecol 2006
Natural Progression of CSP • Towards serosal layer or uterine cavity. • Formerneeds immediate intervention due to high risk of life-threatening bleeding and uterine rupture. • In the latter, conservative management, till viability has been attempted Ash A et al. BJOG 2007 Litwicka K et al. CurrOpinObstetGynecol2011
Safety of conservative management of CSP • This resulted in uterine rupture, severe hemorrhage and DIC in 3 out of 6 patients, mandating hysterectomy • Severe bleeding complicated remaining three cases, which needed control with salvage treatments. Rotas M et al AJOG 2006
Management of ectopic pregnancies with MTX • Systemic MTX is the standard management for ectopic pregnancies less than 9 weeks gestation, with fetal pole less than 10mm, absent fetal heart activity and serum beta-hCG less than 10,000mIU/ml Rotas M et alObstetGynecol 2006
Outcome of CSPs managed with systemic MTX Of the 16 cases: • Five with ß-hCG less than 5000mIU/ml had complete resolution within a few months. • Another five received multiple doses of MTX alternating with folinic acid. • Of these, two needed additional laparotomy and hysterectomy Al-HashmiS et al. BMJ case reports 2012
Other routes of MTX • Due to fibrous scar tissue leading to limited absorption of systemic MTX, intra-gestational sac MTX has also been used especially in women with higher BhCG levels Godin PAet al FertilSteril 1997 JurkovicD et al Ultrasound ObstetGynecol2003
Other agents • Other local embryocides like hyperosmolar glucose, potassium chloride and crystalline trichosanthin have been tried FylstraDL ObstetGynecolSurv 2002 Godin PA et al FertilSteril 1997 MaymonR et al Hum ReprodUpdate 2004
Surgical Management Options • Hysteroscopic coagulation of vessels at implantation site • Laparoscopic removal of gestational mass • Laparotomy with wedge resection of the pregnancy • Ultrasound guided suction evacuation Maymon R et al Hum Reprod Update 2004
Other options for management • Uterine artery embolization along with local or systemic MTX • Blind uterine curettage is contraindicated due to high chances of uterine rupture and severe hemorrhage Maymon R et al Hum Reprod Update 2004 Ash A et al BJOG 2007 Flystra D Obstetrical And Gynecological Survey 2002
Take Home Message • CSP is a potentially serious condition despite advances in many diagnostic techniques and therapeutic measures. • As it is a relatively rare entity and there are no definite guidelines, its management needs to be tailored according to the patient.