Download
1 / 103
1.46k likes | 2.62k Views
Thyroid disorders in children. Rola saad , m.d. unsom. introduction. Thyroid hormone is essential for the growth and maturation of many target tissues, including the brain and skeleton.

E N D
Thyroid disorders in children Rolasaad, m.d. unsom
introduction Thyroid hormone is essential for the growth and maturation of many target tissues, including the brain and skeleton. As a result, abnormalities of thyroid gland function in infancy and childhood result not only in the metabolic consequences of thyroid dysfunction seen in adult patients, but in unique effects on the growth and /or maturation of these thyroid hormone-dependent tissues as well.
introduction There are critical windows of time for thyroid hormone-dependent development and so the specific clinical consequence of thyroid dysfunction depends on the age of the infant or child.
introduction In the newborn infant, thyroid function is influenced not only by the neonate’s own thyroid gland but by the transplacental passage from the mother of factors that affect the fetal thyroid gland.
introduction For example, newborn infants with congenital hypothyroidism frequently have hyperbilirubinemia, and delayed skeletal maturation, reflecting immaturity of liver and bone, respectively, and they are at risk of permanent mental retardation if thyroid hormone therapy is delayed or inadequate; their size at birth, however, is normal.
introduction In contrast, hypothyroidism that develops after the age of three years (when most thyroid hormone-dependent brain development is complete) is characterized predominantly by a deceleration in linear growth and skeletal maturation but there is no permanent effect on cognitive development.
Inactivating pathway (D3, D1) Activating pathway (D1, D2) Increased in sick euthyroid 80% conversion from T4 & 20% secreted
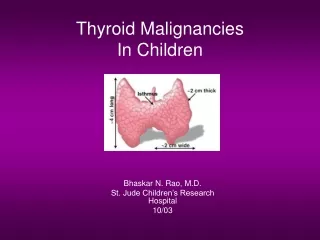
Embryology of the Thyroid Gland Week 7-Fetal thyroid = epithelial bud from the foramen cecum. During descent into neck: -Lateral evaginations of 4th pharyngeal pouch (C-cell ultimobranchial bodies-neural crest origin), fuse with the Thyroid. -The thyroid develops lateral lobes. Week 9-Completes descent into the neck attached to the thyroglossal duct . Weeks 10-12-Obliteration of thyroglossal duct –embryogenesis Complete with development of the bilobar thyroid, folliculogenesis and terminal differentiation of thyroid cells with TSH receptors takes place. TSH Not Required
Pituitary-Thyroid function Maturation Hypothalamic-pituitary Axis 20 wk Iodide transport and trapping 10 wk Secretion T3, T4, TSH 12 wk Wolff-Chaikoff effect matures 36 wk Thyroid Development, descent 7-12 wk 3200 10 20 30 40 Maternal T4 important Gestational Age (Weeks)
Developmental Genes & Transcription factors: TTF-1 (Nkx2.1)—Homeodomain family– thyroid, brain and lung-Homozygosity in mouse—thyroid agenesis, lung hypoplasia, severe brain abnormalities —Heterozygous human mutations— choreoathetosis, pulmonary lesions, and mild hypothyroidism. NKX2.5-Thyroid dysgenesis, cardiac malformations (explanation for increase in cardiac malformations?). TTF-2 (Foxe1)-–Forkhead TF –thyroid, palate-mice have ectopic thyroid or athyreosis + cleft palate-homozygous human mutations-athyreosis, cleft palate, choanal atresia, spiky hair. PAX8-paired domain TF-thyroid, kidney, embryonic brain mice have athyreosis, heterozygous PAX8 human mutants have variable eutopic thyroid hypoplasia and cysts-important for TPO transcription, occasional renal agenesis.
Developmental GenesTranscription factors: To date only 2% of congenital hypothyroidism secondary to thyroid dysgenesis is familial. Very few of these infants have an identified transcription factor mutation.
Thyroid Hormone Action T3 binds to two nuclear receptors, encoded by separate genes with multiple isoforms (alternative splicing): TRα1 TRα2 (does not bind to T3). TRβ-1 TRβ-2 TRβ-3. Nuclear receptors with bound T3 then bind to regulatory elements in thyroid hormone responsive genes. Those without bound T3 may suppress T3 action. Tissue specificity: TRβ –Liver, muscle, kidney predominate. TRβ2—high in hypothalamus, pituitary. TRα—predominates in brain.
Congenital Hypothyroidism-Etiology Thyroid dysgenesis/agenesis due to a developmental problem: Rarely associated with gene defects. Thyroid dyshormonogenesis. Resistance to TSH binding or action (TSH receptor or G-protein mutation-PHP 1a). Secondary Hypothyroidism (Central): TRH deficiency– can be anatomic. TSH deficiency (Beta subunit mutation). TRH resistance (TRH receptor mutation). Pituitary transcription factor defect: HESX1, LHX3, LHX4, PIT1, PROP1 mutations.
Congenital Hypothyroidism-Etiology Peripheral Hypothyroidism Thyroid hormone resistance or transport defect (MCT8.) Syndromes. Transient Maternal Goitrogens. Maternal TSH receptor blocking abs. Iodine deficiency or excess. Heterozygous THOX2 or DUOXA2. Congenital Hemangioendothelioma (consumption because of reverse deiodinase excess).
Thyroid Hormones and TSH—Fetus and Neonate TSH --surge in response to hypothermia within 30 min of delivery is attenuated in low birthweight infants. T4 (and FT4)--rises In response to the TSH surge, peaking at day 7 in AGA infants, later in LBW. T3-rises after birth, peaking after 2-4 weeks— because of TSH rise and response to shift in ring deiodinases ( inc Type 1, dec type 3)-rise is less prominent in LBW infants. rT3-decreases after birth, dropping by 1 week from very high levels. TBG—increases with age, lower in LBW infants.
Thyroid Hormone Transport 80% of circulating T3 produced by extrathyroidal conversion of T4. 20% from thyroid secretion. T4 and T3 diffuse into cells or are actively transported ( as in brain). Defects in the MCT8 thyroid transporter cause severe neurologic impairment—this is an X-linked disorder associated with elevated T3, low T4 and normal TSH.
Hypothyroidism Screening in the Newborn Programs vary– most check heel stick T4 and follow with TSH in all or in a certain percent (lowest 10-20%) of screened infants. Because of the rapid changes in T4 and TSH in the first few days of life, it is important to take into account when the sample is obtained. Some programs check in follow up in 2-4 weeks. Different criteria must be employed for LBW babies. Use the published AAP Guidelines for detection and follow up: S.R. Rose, R.S. Brown, T. Foley, P.B. Kaplowitz, C.I. Kaye and S. Sundararajan et al., Update of newborn screening and therapy for congenital hypothyroidism, Pediatrics 117 (2006), pp. 2290– 2303.
Hypothyroidism Screening in the Newborn (New Information): -One third or more of infants require follow up at more frequent intervals in the second six months of life than suggested in this guideline: Bharti, Misra, Levitsky, Clinical Monitoring Guidelines for Congenital Hypothyroidism: Laboratory Outcome Data in the First Year of Life, J Pediatr, 2011:158:532-537 -Confirmation of the delayed rise in TSH and potential to miss congenital hypothyroidism in a large cohort of LBW and VLBW infants strongly suggests close follow up and repeat testing in this group: Woo HC, Lizarda A, Tucker R, et al., Congenital hypothyroidism with a delayed thyroid-stimulating hormone elevation in very premature infants: incidence and growth and developmental outcomes,J Pediatr. 2011,158:538-42.
Diagnostic Studies Repeat laboratory measures of TSH, T4 and FreeT4 Think about: Bone age radiograph—knee epiphysis (more likely to be absent in boys Tc v. 123I – easier to get Technecium U/S will tell if thyroid eutopic, and can be used as a f/u if no uptake on scan Thyroglobulin Urine Iodine
Therapy • Replacement therapy with L-thyroxine sodium should be begun as soon as the diagnosis of congenital hypothyroidism is confirmed. • In babies whose initial results on newborn screening are suggestive of severe hypothyroidism (e.g., T4 <5 mcg/dL 64 nmol/L) and/or TSH >50 mU/L), therapy should be begun immediately without waiting for the results of the confirmatory serum. • As noted above, treatment need not be delayed in anticipation of performing thyroid imaging studies as long as the latter are done within 5-7 days of initiating treatment (before suppression of the serum TSH).
Therapy • Parents should be counseled regarding the causes of congenital hypothyroidism, the importance of compliance and the excellent prognosis in most babies if therapy is initiated sufficiently early and is adequate and educational materials should be provided. • An initial dosage of 10-15 ug/kg is generally recommended so as to normalize the T4 as soon as possible. A recent study in a small group of patients has suggested that an even higher initial dose (12 to 17 ug/kg, equivalent to 50 ug in a full term baby) may be even better.
Therapy • Babies with mild hypothyroidism should be started on the lower dosage, while those with severe CH (e.g., T4 <5 ìg/dL (64 nmol/L)), such as those with thyroid agenesis, should be started on the higher dosage. Thyroid hormone may be crushed and administered with juice or formula, but care should be taken that all of the medicine has been swallowed. Thyroid hormone should not be given with substances that interfere with its absorption, such as iron, soy, or fiber. • Many babies will swallow the pills whole or will chew the tablets with their gums even before they have teeth. • Reliable liquid preparations are not available commercially in the US, although they have been used successfully in Europe.
therapy • The aims of therapy are to normalize the T4 as soon as possible, to avoid hyperthyroidism where possible, and to promote normal growth and development. When an initial dosage of 10-15 ug/kg is used, the T4 will normalize in most infants within 1 week and the TSH will normalize within 1month. When a higher dosage is used (12-17 ug/kg) normalization is even faster (3 days and 1 week, respectively). • Subsequent adjustments in the dosage of medication are made according to the results of thyroid function tests and the clinical picture. Often small increments or decrements of L-thyroxine (12.5 ug) are needed. This can be accomplished by 1/2 tablet changes, by giving an alternating dosage on subsequent days, or by giving an extra tablet once a week.
Therapy • Some infants will develop supraphysiologic serum T4 values on this amount of thyroid replacement but the serum T3 concentration usually remains normal, affected infants are not symptomatic, and available information suggests that these short-term T4 elevations are not associated with any adverse effects on growth, bony maturation, or cognitive development.
Therapy • A persistently elevated serum TSH level associated with a normal or increased serum T4 concentration is seen less often now than in the past, possibly because of the higher initial L-thyroxine dose employed. • Relative pituitary resistance has been implicated as a cause of this finding, but noncompliance should always be excluded. • In these cases, the T4 value is used to titrate the dosage of medication. One usually aims to maintain the T4 above 10 ug/dL(128.7nmol/L) and the TSH at less than 10 mU/L. • Close follow-up is necessary. Current recommendations are to repeat the T4 and TSH at 2 and 4 weeks after the initiation of L-thyroxine treatment, every 1-2 months during the first year of life, every 2-3 months between 1 and 3 years of age, and every 3-12 months thereafter until growth is complete. • In hypothyroid babies in whom an organic basis was not established at birth and in whom transient disease is suspected, a trial off replacement therapy can be initiated after the age of 3 years when most thyroxine-dependent brain maturation has occurred.
Therapy • Whether or not premature infants with hypothyroxinemia should be treated remains controversial at the present time. • In the meantime, it would seem reasonable to treat only premature infants with hypothyroxinemia and a normal TSH only in the context of a clinical trial. • In all premature every effort should be made to assure adequate iodine intake, treat the primary illness and to avoid, if possible, drugs (e.g.,dopamine, steroids, aminophylline, caffeine and diamorphine) that have been shown to suppress TSH, with close follow up of circulating thyroid hormone levels until they normalize. Whether or not these infants should be treated with T4 and at what dosage remains to be determined.
prognosis • Although all are agreed that the mental retardation associated with untreated congenital hypothyroidism has been eradicated by newborn screening, controversy persists as to whether subtle cognitive and behavioral deficits remain, particularly in the most severely affected infants. • Both the initial treatment dose (at least 10ug-15 ug/kg) and early onset of treatment (before 2 weeks) are important. Time to normalization of circulating thyroid hormone levels, the initial free T4 concentration, maternal IQ, socioeconomic and ethnic status have also been related to outcome.
prognosis • The long term problems for these babies appear to be in the areas of memory, language, fine motor, attention and visual spatial. • Inattentiveness can occur both in patients who are overtreated and those in whom treatment was initiated late or was inadequate. • In addition to adequate dosage, assurance of compliance and careful long term monitoring are essential for an optimal developmental outcome. • Combined therapy with T4 and T3 offers no advantage to T4 alone.
Causes of acquired hypothyroidism • Central hypothyroidism: • – Intracranial masses • – Panhypopituitarism • – Develop during treatment for GH deficiency • Primary Hypothyroidism: • – Ectopic thyroid gland • – Drugs • – Neck Irradiation • – Iodine deficiency and excess • – Autoimmune hypothyroidism • – Cystinosis
Medications associated with hypothyroidism • Thionamides • – PTU • – Methimazole • – Carbimazole • Sulfonamides • – Sulfisoxazole • – Sulfamethoxazole • Lithium • Anti-seizure medications (phenobarbital, phenytoin and • carbmazepine) • Amiodarone • Radiation
Clinical manifestations • • Central hypothyriodism • Symptoms • Signs of intracranial process • Evidence for additional hypothalamic/pituitary deficiencies • Abnormalities of MRI scan • • Primary Hypothyroidism • Symptoms • Effect on growth and puberty • Deceleration of linear growth velocity • Continued weight gain • Galacctorhea– secondary to elevated prolactin
Clinical manifestations • The onset of hypothyroidism in childhood is insidious. Affected children often are recognized either because of the detection of a goiter on routine examination or because of a poor interval growth rate present for several years prior to diagnosis. • Because the deceleration in linear growth tends to be more affected than weight gain, these children are relatively overweight for their height, although they rarely are significantly obese. • If the hypothyroidism is severe and longstanding, immature facies with an underdeveloped nasal bridge and immature body proportions (increased upper-lower body ratio) may be noted. • Dental and skeletal maturation are delayed, the latter often significantly. Patients with central hypothyroidism tend to be even less symptomatic than are those with 1o hypothyroidism.
Clinical manifestations • The classical clinical manifestations of hypothyroidism can be elicited on careful evaluation, though they often are not the presenting complaints. • These include lethargy, cold intolerance, constipation, dry skin or hair texture, and periorbital edema. • School performance is not usually affected, in contrast to the severe irreversible neuro-intellectual sequelae that occur frequently in inadequately treated babies with congenital hypothyroidism.
Clinical manifestations • Although the surface of the thyroid gland in autoimmune hypothyroidism is classically described as ‘pebbly’ or bosselated, occasionally asymmetric enlargement occurs and must be distinguished from thyroid neoplasia. • A palpable lymph node superior to the isthmus (‘Delphian node’) is often found and be confused with a thyroid nodule. • The thyroid gland, in thyroid hormone synthetic defects, • on the other hand, tends to be softer and diffusely • enlarged. • A delayed relaxation time of the deep tendon reflexes may be appreciated in more severe cases.
Sequential changes in physical appearance in a young girl who presented at 15 years of age with amenorrhea and hyperprolactinemia secondary to severe hypothyroidism. Note her poor linear growth since at least 11 years of age.