Download
1 / 47
490 likes | 826 Views
Outcomes in Decision Analysis: Utilities, QALYs & DALYs, and Discounting. DCEA 24 January 2013 James G. Kahn. Overview. Back to the aneurysm example: To Clip Or Not To Clip? Clinical Outcomes Utilities and utility measurement Direct Indirect QALYs (& DALYs)

E N D
Outcomes in Decision Analysis: Utilities, QALYs & DALYs, and Discounting DCEA 24 January 2013 James G. Kahn
Overview Back to the aneurysm example: To Clip Or Not To Clip? Clinical Outcomes Utilities and utility measurement Direct Indirect QALYs (& DALYs) Discounting
Review—Last Lecture Formulated an explicit question “to clip or not to clip” (incidental aneurysm) Made a simple decision tree Conducted an expected value calculation to determine which course of action would likely yield the highest life expectancy
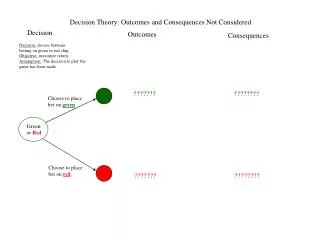
To Clip or Not To Clip =.9921 =.55 =1.0 =.55 =.977 Diff = -0.0151 =0 .865 vs .977
To Clip or not to Clip? • Has an impact on life expectancy • Also actual clinical outcomes: • Surgical death • Aneurysm rupture • Death from aneurysm rupture • Neurologic Injury • Major • Minor • Fear of aneurysm rupture
Quantifying Health Outcomes • Mortality • Life Years number of expected years of life • Significant Morbidity Paralysis, loss of sight • Quality Adjusted Life Years Life years adjusted for value of health state • Disability Adjusted Life Years Disease burden – lost years + disability • Financial Valuation of Outcomes Costs to patient, payer, or society Willingness to pay to avoid outcomes
Health Outcomes – Mortality • Mortality Death from disease/accident/procedure e.g. If Ms. Brooks undergoes surgery, one of the possible outcomes is mortality • Life Years Calculate an expected value of life years using a probabilistically weighted average of expected life e.g. If Ms. Brooks does not undergo surgery, her life expectancy is less than if she did not have aneurysm, these outcomes are measured in expected life years
Health Outcomes – Morbidity • Morbidity Some health state that is less than perfect e.g. disability from stroke, chronic pain • Comparison of morbidities Difficult – apples and oranges problem e.g. which is worse: Blind v. Deaf Deaf v. Paraplegia Paraplegia v. Blind
To Clip or not to Clip? • Clinical outcomes for clinician readers • Outcomes may affect health-related quality of life: how do we compare? • Neurologic injury can cause mild/moderate disability • Not clipping can cause anxiety associated with being at risk of aneurysm rupture • Outcomes may occur at different times
How do we incorporate quality-of-life effects into decision analysis? • Measure/estimate and apply health state utilities • Use utilities to quality-adjust life expectancy for decision and cost-effectiveness analysis
Preview—Where We Are Going with this Analysis? Recall Ms. Brooks and her incidental aneurysm -- to clip or not to clip? We want to: Determine her utilities Use them to generate QALYs Evaluate incremental QALYs and cost (CEA/CUA) Compare incremental cost effectiveness ratios (ICER) to other currently accepted medical interventions
What is a Utility? Utility - Quantitative measure of the strength of an individual’s preference for a particular health state or outcome. Utilities can be obtained for: * Disease states (diabetes, depression) * Treatment effects (cure, symptom management) * Side effects (impotence, dry mouth) * Process (undergoing surgery, prenatal diagnostic procedure)
Utilities Utilities are the currency we use to assign values to outcomes Scaled from 0 to 1 1 = perfect or ideal health or health in the absence of the condition being studied 0 = death
How are utilities measured? Direct – compare with 0 / 1 anchors - Visual Analog Scale - Standard Gamble - Time Trade-off Indirect Assess standard health domains (e.g., physical functioning, pain, and cognition) and calculate 0-1 utility with an equation.
BKA vs. AKA Example Patient in hospital has infection of the leg Two options: 1) BKA – below knee amputation BKA –1% mortality risk 2) Medical management – 20% chance of infection worsening and needing AKA (above the knee amputation), 10% mortality risk
For which outcomes do we need to measure utilities? • Living without part of a leg (below the knee) • Living without a bigger part of a leg (above the knee) • Pain • Worry • Other
Visual Analog Scale Full health: intact leg 100 98 99 65 BKA 55 AKA 2 1 Dead 0 Outcomes rated on a 0-to-100 “feeling thermometer.”
Standard Gamble What chance of immediate death would you be willing to incur to avoid living with the outcome being assessed? Method relies on respondents choosing between: 1) a certain outcome (BKA) 2) a gamble between an ideal outcome (intact leg) and the worst outcome (dead)
Standard Gamble Question Death Perfect Health
Standard Gamble Exercise Which do you prefer? Choice A Choice B Spend the rest of your life with BKA [p]% chance of immediate death 1-[p]% chance of spending the rest of your life with an intact leg
Standard Gamble • Standard gamble measurement involves questioning patients to determine the p at which the two outcomes are equivalent • Using expected utilities, the value of p implies the utility • Utility (BKA) x Prob (BKA) • = Utility(cure) x (1-p) + Utility(death) x (p) • Thus, if utility of cure = 1 and of death = 0, the utility of BKA = 1-p.
Time Tradeoff How many years of your life would you be willing to give up to spend your remaining life without the condition/health state being assessed? Method relies on respondents choosing between: 1) Full life expectancy with the condition/outcome being assessed (BKA) 2) A reduced life expectancy with the ideal outcome (intact leg)
Time Tradeoff Preference Elicitation Which do you prefer? Choice A Choice B Spend the remaining 40 years of your life with BKA Live 40 more years of life with an intact leg (give up 0 years of life)
Time Tradeoff Preference Elicitation Which do you prefer? Choice A Choice B Spend the remaining 40 years of your life with BKA Live 30 more years of life with an intact leg (give up 10 years of life)
Utility Measurement – Time Trade-off Find years of life at which patient is indifferent between Choice A (with health problem) & Choice B (shorter life). We assume that: Time A * Utility A = Time B * Utility B And thus Utility A = [Time B * Utility B] / Time A If willing to give up 4 years to avoid BKA: Utility of BKA = [(40-4) * 1] / 40 = 36/40 = 0.9
Pros and Cons - VAS Advantage: Easy to understand Disadvantages: Doesn’t require the respondent to: - Think about what they’d be willing to give up - Explore risk preference Values spread over the range
Pros and Cons – SG Advantages: Requires assessor to give something up, incorporates risk attitude Disadvantages: Choices may be difficult to make Most confusion-prone method Lack of engagement or willingness to participate in exercise Utility values tend to cluster near 1
Pros and Cons – TTO Advantages: Still asking assessor to give something up Easier choices than SG. Values not so clustered near 1 Disadvantages: Fails to incorporate risk Lack of clarity of when time traded occurs Isn’t something that one can choose to give up. (One can take on a risk of death, but not “pay with life years.”)
Indirect measures of utility First assess features of health using standard domains (attributes) respondents complete a questionnaire Then calculate utility (0 - 1) with equation score using a “multi-attribute scoring function” derived from community preferences for health states defined by these attributes
Utilities in decision analysis Utilities are used to add morbidity effects to life expectancy. Quality Adjusted Life-Years (QALYs) (we’ll return to DALYs later)
QALYs QALYs are usually considered the standard unit of comparison for outcomes for CEAs in OECD QALYs = time (years) x quality (utility) e.g. 40 years life expectancy after AKA, utility (AKA) = 0.9 = 40 x 0.9 = 36 QALYs (undiscounted) Mortality lowers LY, morbidity lowers QA
Including utility for early death and disability due to stroke
Outcomes - Discounting Aneurysm Example We said since life expectancy is reduced by 2/3, so instead of 35, it is = 35 * .333 = 11.67 However, are all years considered equal? Consider: Favorite Meal Extreme Pain Lifetime Income
Outcomes - Discounting Generally, present value more than future One way to value the different times is discounting Essentially this year is worth D more than next year D (annual discount rate) usually set at 3% To compare values of all future times, a calculation, net present value, is often used NPV = 1 / (1 + D)t Where t is number of years in the future
Outcomes - Discounting Aneurysm Example If utility is 0.6 and life expectancy is 3 years NPV would be: Utility / (1 + D)t or NPV = 0.6 / 1 + 0.6 / (1.03)1+ 0.6 / (1.03)2 However, since events in year 1 occur on average half way through, we can use 0.5 for year 1: NPV = 0.6 / (1.03)0.5 + 0.6 / (1.03)1.5 + 0.6 / (1.03)2.5
QALYs vs. DALYs • “Quality Adjusted Life Years” (QALYs) • came first; still used for CEAs in OECD • measure of health. • An illness which shortens life by 2 years and lowers “health status utility” by 20% for 5 years decreases QALYs by -2 - 0.2 * 5 = -3 • Interventions are designed to increase QALYs • “Disability Adjust Life Years” (DALYs) • most common health metric in global health. • measure of disease burden – i.e., the negative of QALYs. • An illness which shortens life by 2 years and raises “disability” by 20% for 5 years increases DALYs by 2 + 0.2 * 5 = 3 • Interventions are supposed to avert DALYs.
* In practice, methods to estimate disability weight and health status utility often overlap, relying on similar elicitation of expert or patient or population opinion.
Exponential Discounting • Exponential discounting first described in 1937* • Mathematically easy to manipulate • Assumed discounting in “simple regular fashion” • Does not differentiate difference between: • Today vs. tomorrow • Ten years vs. ten years plus one day *Samuelson PA. A Note on Measurement of Utility. Rev Econ Stud 1937;4:155-61
Overall Review Outcomes - Clinical Mortality - timing Morbidity – severity, duration, timing Measuring Utilities Direct – TTO most often Indirect – may underestimate utility QALYs - health, DALYs – disease burden Discounting NPV = Utility / (1 + D)t