Download
1 / 67
680 likes | 967 Views
A Focus On Chlamydia screening. Susan DeLisle , ARNP, MPH National Chlamydia Coalition Partnership for Prevention. Outline. The National Chlamydia Coalition Why Chlamydia Screening is a HEDIS Measure Epidemiology of Chlamydia Why Care About Chlamydia Disease outcomes

E N D
A Focus On Chlamydia screening Susan DeLisle, ARNP, MPH National Chlamydia Coalition Partnership for Prevention
Outline • The National Chlamydia Coalition • Why Chlamydia Screening is a HEDIS Measure • Epidemiology of Chlamydia • Why Care About Chlamydia • Disease outcomes • Cost Implications for health plans • National HEDIS and other performance data • Perceived Barriers to Screening • Resources and Tools
National Chlamydia Coalition (NCC) • Formed in 2008 • Comprised of over 40 organizations • Health care professional organizations • Insurers • Non-profit organizations • Local, state, federal government representatives • Managed by Partnership for Prevention • Funded by the Centers for Disease Control and Prevention
National Chlamydia Coalition: • Mission • Address the high burden of chlamydia in adolescents and young adults by promoting equal access to comprehensive and quality health services
Purpose in Attending this Meeting • Learn what’s working and what’s not • Promote chlamydia screening • Exchange ideas to increase chlamydia screening • Provide resources, tools, tips, and assistance
Why Chlamydia Screening is a HEDIS Measure • Cost effective and cost beneficial • Grade A USPSTF Measure for women <25 years of age • Screening works! to prevent long term and costly consequences • Indicator of adolescent and maternal health
The Problem: Chlamydia • Most commonly reported nationally notifiable disease in the US • Over 1.3 million cases reported in 2010 • Estimated 2.8 million cases occur each year • Direct medical costs: $678 million/year • Often asymptomatic (up to 80% of cases) • Devastating sequelae CDC Sexually Transmitted Disease Surveillance, 2008. Atlanta, GA: U.S. Department of Health and Human Services; November 2009 Weinstock H, Berman S, Cates W Jr. Perspect Sex Reprod Health 2004 Chesson HW, et al. Perspect Sex Reprod Health 2004
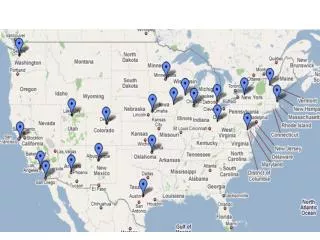
Chlamydia—Rates by State, United States and Outlying Areas, 2010 NOTE: The total rate of chlamydia for the United States and outlying areas (Guam, Puerto Rico, and Virgin Islands) was 422.6 per 100,000 population.
Burden of Infection Sexually active people aged 14-24 have about 3x the chlamydia prevalence of sexually active adults aged 25-39 Prevalence, % Age group (years) NHANES, National Health and Nutrition Examination Survey, 1999-2008 Sexual activity =“yes” response to “Have you ever had sex?” Sex = vaginal, anal, or oral sex 9
Chlamydia Prevalence in Sexually Active Females Aged 14-24 in the United States Prevalence, % NHANES, National Health and Nutrition Examination Survey, 1999-2008 Sexual activity =“yes” response to “Have you ever had sex?” Sex = vaginal, anal, or oral sex 10
Chlamydia—Percentage of Reported Cases by Sex and Selected Reporting Sources, United States, 2010 *HMO = health maintenance organization; HD = health department. NOTE: These categories represent 72.5% of cases with a known reporting source. Of all cases, 11.6% had a missing or unknown reporting source. Percentage 40 Private Physician/HMO* STD Clinic 35 Other HD* Clinic 30 Family Planning Clinic Emergency Room 25 20 15 10 5 0 Men Women
Sequelae: PID and Tubal Factor Infertility infertility • Infectious Complications • Neonatal pneumonia or eye infections in 60-70% of infants born to untreated mothers • At least 2-5 fold increased risk of HIV Infection chlamydia 20% 10-20% ectopic pregnancy pelvic inflammatory disease 9% 10-20% gonorrhea 18% chronic pelvic pain
Pelvic Inflammatory Disease (PID) • Symptoms are often vague • 85 % of women delay seeking medical care for PID • Frequently misdiagnosed because there is no test for PID • Delaying care increases the risk of infertility and ectopic pregnancy
Why Screen Sexually Active Females? • 80%-90% of chlamydial infections in women have no symptoms • Data from a randomized controlled trial of chlamydia screening in a managed care setting suggest that screening programs can lead to a reduction in the incidence of PID by as much as 60% • Reducing the incidence of PID can reduce infertility Scholes D, Stergachis A, Heidrich FE, Andrilla H, Holmes KK, Stamm WE. Prevention of pelvic inflammatory disease by screening for cervical chlamydial infection. N Engl J Med 1996;34(21): 1362-66.
Infertility Services are Costly • Tubal factor infertility, caused by Chlamydia trachomatisor by Neisseriagonorrhoeae, is estimated to affect as many as 18% of women using Assisted Reproductive Technology (ART) • 12% of women in the U.S. ages15-44 have ever used infertility services • Infertility treatments are associated with an increased risk of multiple order births, which carry health risks for women and infants, and increased costs Source: Centers for Disease Control and Prevention, A National Public Health Action Plan for the Detection, Prevention, and Management of Infertility. 2012
Infertility Services are Common • Among women 15-44 • 7.4% are affected by infertility • About 12% have impaired fecundity • Each year, more than 1.1 million women of reproductive age seek medical help to become pregnant • 7.3 million women have received infertility services, including counseling and diagnosis, in their lifetimes Source: Centers for Disease Control and Prevention, A National Public Health Action Plan for the Detection, Prevention, and Management of Infertility. 2012
How Compliant are Providers with Annual Chlamydia Screening? 2010 Chlamydia Screening HEDIS Rates Health Plan Type Age (yrs) Commercial HMO (%) Medicaid HMO (%) _____ ________________ ____________ The State of Health Care Quality, 2011 National Center for Quality Assurance at: http://www.ncqa.org/LinkClick.aspx?fileticket=J8kEuhuPqxk%3d&tabid=836
HEDIS Chlamydia Measure • # Eligible women receiving chlamydia screening # Sexually active women, aged 16-24 • Measure collected separately for women 16-20 and 21-24
Barriers to Screening Women in Private Sector Settings • Policy • Absent or conflicting chlamydia screening guidelines or policies • System • Competing priorities, lack of time or staff, cost effectiveness • Lack of reimbursement • Provider • Belief that chlamydia prevalence in population is low • Discomfort with taking sexual history • Patient • Low perception of risk, not aware of asymptomatic infection • Concerns about confidentiality
Health Care Reform • Affordable Care Act provides full health plan coverage for U.S. Preventive Services Task Force (USPSTF) A and B graded preventive health services with no cost sharing • Chlamydia screening all sexually active females under 25 years is a USPSTF Grade A recommendation
Opportunities for STD Screening and Treatment • New (time-saving) tools • Easy and inexpensive methods to increase screening rates • New tests • Vaginal swab samples – self collected • Urine tests for both male and females • Easy treatment • Single dose treatment
Overcoming the Barriers • Evidence based interventions exist to increase screening rates • Next speaker will discuss a proven model to address Chlamydia screening • Model can apply to other HEDIS measures
Other Evidenced Based Interventions • NCC mini grants • Used evidenced based best practices in a variety of health care settings: • Private Pediatric practices • Internal Medicine • Family Practice • Managed Care • Improved Chlamydia screening rates in all settings: • Young women screened increased 8%-22% • Increases in confidential risk assessment, education, and counseling
Common Themes • Engage office staff (not just providers) to elicit barriers and identify solutions • Develop “tool kit” • Information on tests • Tailored risk assessment • Patient and parent education materials • Patient flow • Address Confidentiality • Provide feedback on screening rates, prevalence by practice site
Tools Available • Resources for: • Screening tips and tools • Provider resources • Simple risk assessment tools • Ensuring confidentiality • Addressing billing and EOBs • Patient and parent education materials
Accessing the Tools • Available at: • National Chlamydia Coalition: http://ncc.prevent.org/ • AAP: www.aap.org/moc/AdolHandouts_AAPMbrs/ProviderHandouts.htm • SAHM: www.adolescenthealth.org/Clinical_Care_Resources/2721.htm • ACOG: www.acog.org/goto/teens
Thank You • We’d love to work with you
Practice Models And Resources
Other Evidenced Based Interventions • NCC mini grants • Used evidenced based best practices in a variety of health care settings: • Private Pediatric practices • Internal Medicine • Family Practice • Managed Care • Improved Chlamydia screening rates in all settings: • Young women screened increased 8%-22% • Increases in confidential risk assessment, education, and counseling
Common Themes • Engage office staff (not just providers) to elicit barriers and identify solutions • Develop “tool kit” • Information on tests • Tailored risk assessment • Patient and parent education materials • Patient flow • Address Confidentiality • Provide feedback on screening rates, prevalence by practice site
Tools Available • Resources for: • Screening tips and tools • Provider resources • Simple risk assessment tools • Ensuring confidentiality • Addressing billing and EOBs • Patient and parent education materials
Accessing the Tools • Available at: • National Chlamydia Coalition: http://ncc.prevent.org/ • AAP: www.aap.org/moc/AdolHandouts_AAPMbrs/ProviderHandouts.htm • SAHM: www.adolescenthealth.org/Clinical_Care_Resources/2721.htm • ACOG: www.acog.org/goto/teens
Thank You • We’d love to work with you
Meeting NCQA Goals for Adolescent Chlamydial Screening & Beyond Kathleen Tebb, PhD Division of Adolescent & Young Adult Medicine Department of Pediatrics
Presentation Overview • Discuss preventive health practice guidelines for adolescents & young adults • Present an evidence-based clinical practice quality improvement model • Discuss barriers and strategies to improve chlamydial screening & health quality for adolescents & young adults
Why Improve Delivery of Preventive Care for Adolescents? • Adolescents/parents view clinicians as credible resources & expect guidance • Nearly ¾ of adolescents see a primary care clinician at least 1/year • Growing evidence that motivational interview, counseling & screening promotes healthy behaviors • ACA 2010: accountability, transparency, accreditation
Clinical Guidelines for Adolescent Annual Visit • Primary care clinicians are to screen for risk behaviors& remind adolescents & families about strengths • All adolescents have some time alone with clinicianduring preventive visit
Guideline Implementation • 38% of adolescents have preventive visit. • <10% of adolescents received a basic complement of 6 preventive recommendations. • >50% don’t have time alone with clinician • 30% forgo care in “risky areas” due to confidentiality concerns • Training and screening tools in clinical practice can increase the delivery of preventive services
Methods • Settings: • RCT: Large HMO in Northern California • Preventive Visits • Acute Care Visits • Sustainability • Translatability: HMO and Australia
Clinical Practice Improvement Model Engage Team Building Re-Design Clinical Practice Sustain the Gain
Clinical Practice Improvement Model • Leadership • Best practices • Define gap • Raise Awareness Engage Team Building Re-Design Clinical Practice Sustain the Gain
Clinical Practice Improvement Model • ACTeam • Skill building • Tool Kit Engage Team Building Re-Design Clinical Practice Sustain the Gain
Site Specific Flow Chart Cue Charts Room Patient MD/NP VISIT Urines To Lab Follow-Up ID eligible teens Stamp charts Urine collection Assess risk Preventive counsel If SA+ Lab req confid. # RN contacts CT + teen Teen comes to clinic for Rx RN enters Rx in STD log book MA refrigerates urines MA enters teen name, confidential # in log book • Runner takes urines to lab
Clinical Practice Improvement Model Engage • Customize • Measure success Team Building Re-Design Clinical Practice Sustain the Gain