Download
1 / 60
690 likes | 1.54k Views
Clinical Problems in the Postanesthesia Recovery Room (PACU). Heidi Eriksson, MD, PhD Helsinki University Central Hospital Finland. Recovery room incidents: a review of 419 reports from the Anaesthetic Incident Monitoring Study (AIMS) Kluger and Bullock Anaesthesia 2002.

E N D
Clinical Problems in the Postanesthesia Recovery Room (PACU) Heidi Eriksson, MD, PhD Helsinki University Central Hospital Finland
Recovery room incidents: a review of 419 reports from the Anaesthetic Incident Monitoring Study (AIMS) Kluger and Bullock Anaesthesia 2002 • The Australian incident monitoring study (Anesthesia and Intensive Care 1993) • incident reporting study • voluntary, self-reporting audit of actua/potential incidents that occur during anesthesia • 8372 reports , 478´(18%) in PACU
Recovery room incidents: a review of 419 reports from the Anaesthetic Incident Monitoring Study (AIMS) • 92 % in adults • 90 % during daytime hours • 4 % at night Kluger and Bullock. Anaesthesia 2002
Factors influencing stay in the postanesthesia care unit Seago J et al. J Clin Anaesth 1998 • Patient history and age were not predictive! • Postoperative pulmonary/airway problems • desaturation, stridor, obstruction • Postoperative cardiovascular problems • hypo/hypertension, chest pain/ECG changes, pulmonary oedema/HF • Length of surgery • Unexplained - due to organizational factors ??
American Society of Anesthesiologists-Physical Status Classification(ASA-PS) • is not an indicator of perioperative risk • Perioperative risk • preoperative medical status • nature on the anesthetic technique • nature of the surgical procedure low risk- intermediate risk- high risk • does not take into account • age • complexity of the operation • is a measure of preoperative medical status
Type of procedure & recovery room incidents reported to AIMS General surgery 118 28 % Orthopedics 72 17 % Ear, nose and throat 42 10 % Opthalmology 33 8 % Gynecology 30 7 % Urology 28 7 % Vascular 25 6 % Dental and maxillofacial 14 3 % Plastic 12 3 % Cardiothoracic 12 3 % Obstetric 10 2 % Electroconvulsive 6 1 % Neurosurgery 5 1 % Pain block 2 0.5 % Radiology 1 0.2 % Vascularaccess 1 0.2 % Kluger and Bullock. Anaesthesia 2002
Primary presenting problem & recovery room incidentsreported to AIMS Cardiovascular 99 24 % Respiratory 97 25 % Airway 86 21 % Drug error 44 11 % CNS 32 8 % Equipment 27 6 % Communication problems 7 2 % Hypotermia 6 1 % Regional block problems 4 1 % Inadequate documentation 4 1 % Hyperthermia 3 1 % Trauma 3 1 % Dental problems 2 0.5 % Renal 1 0.2 % Skin 1 0.2 % Blood transfusion 1 0.2 % Facility limitations 1 0.2 % Gastrointestinal problems 1 0.2 % Kluger and Bullock. Anaesthesia 2002
Presenting problem in 99 cardiovascular incidents out of 419 PACU incidents reported to AIMS Pulmonary oedema 29 7 % Hypotension 26 6 % Cardiac arrest 20 5 % Bradycardia 7 2 % Myocardial ischemia 7 2 % Tachycardia 4 1 % Bleeding 2 0.5 % Hypertension 2 0.5 % Allergy 1 0.2 % Radial artery ischemia 1 0.2 % Kluger and Bullock. Anaesthesia 2002
Hypotension in PACUQuick assessment • decreased ventricular preload • hypovolaemia • postoperative bleeding • reduced myocardial contractility • myocardial ischemia • congestive heart failure • reduction of systemic vascular resistance • septicaemia • regional anesthesia/analgesia • anaphylaxis
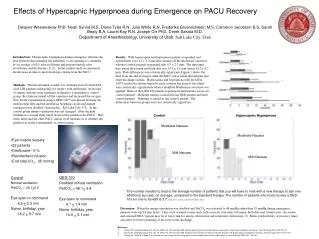
Hypertension in PACUQuick assessment • pain • hypoxia • hypercapnia • anxiety/agitation • fluid overload • developing pulmonary oedema • urinary retention • untreated hypertension
Heart rhytm abnormalities in PACUQuick assessment • pain • hypoxia • hypercapnia • hypovolaemia/hypervolaemia • electrolyte inbalance • metabolic acidosis • pre-existing heart disease • myocardial ischemia
Presenting problem in 97 respiratory incidents out of 419 PACU incidents reported to AIMS Respiratory failure: inadequate oxygenation/ventilation 74 18 % Aspiraton 7 2 % Respiratory arrest 6 1 % Bronchospasm 5 1 % Pneumothorax 5 1 % Kluger and Bullock. Anaesthesia 2002
Presenting problem in 97 airway incidents out of 419 PACU incidents reported to AIMS Airway obstruction 59 14 % Laryngospasm 18 4 % Jaw dislocation 2 0.5 % Foreign body (throat pack) 2 0.5 % Failed extubation 1 0.2 % Endobronchial intubation 1 0.2 % Kluger and Bullock. Anaesthesia 2002
Desaturation in PACUQuick assessment • airway obstruction • laryngeal spasm • bronchospasm • hypoventilation • obesity • perfusion-ventilation • atelectasis • pulmonary oedema • pneumothorax • pulmonary embolism • aspiration • pain
Hypoventilation in PACUQuick assessment • oversedation • residual anesthetic • opioids • parenteral • epidural/intrathecal
Wheezing in PACUQuick assessment • laryngeal spasm (stridor) • after thyroid operation • bleeding • paresis of n recurrens • bronchospasm • asthma • bronchial hyper-responsivess (smoking, postviral) • pulmonary oedema • aspiration • anaphylaxis
But does residual neuromuscular block put our patients in danger? • Muscle function and coordination of protective reflexes of the pharynx and upper esofagus recover late • Eriksson L et al. Anesthesiology 1997 • Ventilatory response to hypoxia is reduced (direct inhibition of chemoreceptor activity in the carotic bodies) • Eriksson L et al. Anesthesiology 1993, Wyon N et al Anesthesiology 1999 • Volunteers • Difficulty in maintaining airway • Desaturation and need for supplemental oxygen • Disability to swallow • Distress • PACU time prolonged • Murphy et al. Anesth Analg 2004 • Eikerman et al. Anestehsiology 2003 • Kopman A et al. Anesthesiology 1997 • Bissinger et al. Physiol Res 2000
Residual neuromuscular block is a risk factor for postoperative pulmonary complications: A prospective, randomised, and blinded study of postoperative pulmonary complications after atracurium, vecuronium and pancuroniumBerg et al. Acta Anaesthesiol Scand 1997 • Manual TOF during operation • TOF 1-2/4 • Reversal when 2-4/4 • Extubation when 4/4 • Mechanomyographically postoperatively • Follow-up up to 6 PODs • Postoperative pulmonary complication : pneumonic infiltration/atelectasis in X-ray
TOF recordings at first postoperative mechanomyographic recording Berg et al. Acta Anaesthesiol Scand 1997
Postoperative pulmonary complications Berg et al. Acta Anaesthesiol Scand 1997
Type of surgery and the risk of pulmonary complications Berg et al. Acta Anaesthesiol Scand 1997
Probability of postoperative pulmonary complications Berg et al. Acta Anaesthesiol Scand 1997 Multiple logistic regression analysis relating the probability of POPC to various covariates
Residual paralysis in the PACU after single intubating dose of nondepolarizing muscle relaxant with an intermediate duration of action Debaene et al Anesthesiology 2003 • 526 patients • 2ED95 dose of vecuronium, rocuronium, or atracurium • No muscle relaxant thereafter • Excluded, if reversal used • Time delay between the injection of muscle relaxant and quantitative measurement of neuromuscular blockade assessed
Conclusion: A long duration between the administration of a single dose of an internediate-acting nondepolarizing muscle relaxant and the arrival to PACU does not guarantee the lack of residual paralysis Note! hypothermia, halogenated anesthesia agents Bedaene et al. Anesthesiology 2003
Residual neuromuscular block Widely used tests to assess recovery from neuromuscular block • Train-of-four ratio > 0.7 / 0.9 by peripheral nerve stimulation • Reliable clinical tests of postoperative neuromuscular recovery • Sustained head lift fot 5s • Sustained leg lift fot 5 s • Sustained hand grip for 5 s • Sustained tongue depressor test • Maximun ispiratory presuure >-50 cm H20 However, poor sensitivity do not secure against residual block ! Pedersen et al. Anesthesiology 1990 Shorten et al. Can J Anaesth 1995 Fruergaard et al. Acta Anaesthesiol Scand 1998 Bedaene et al. Anesthesiology 2003
Residual neuromuscular block • Significant residual block can be excluded only by objective, methods • mechanomyography • electromyography • acceleromyography • ”It is time to move from discussion to action and introduce objective neuromuscular monitoring to all ORs. I believe that objective neuromuscular monitoring is an evidence-based practice and should consequently be used whenever a nondepolarizing neuromuscular blocking agent is administered” Eriksson L. Evidence-based practise and neuromuscular monitoring. It,s time for routine quantitative assessment. Anesthesiology 2003
”The ideal world is one thing, and the real world another!” Viby-Mogensen. Postoperative residual curarization and evidence-based anaesthesia. BJA 2000
How to avoid residual neuromuscular block? (I) • Long acting neuronuscular blocking agents should not be used • Antagonizethe block at the end of the procedure • Reversal initiated only when (2-)3-4/4 TOF stimulations present or when spontaneous muscle activity is present • Prefer tactile evaluation of response to double-burst stimulation (DBS) to TOF stimulation • Consider clinical signs and symptoms in relation to the response to nerve stimulation • Keep in mind the additive/prolonged effects caused by anesthetics and hypothermia Viby-Mogensen. Postoperative residual curarization and evidence-based anaesthesia. BJA 2000
How to avoid residual neuromuscular block? (II) • Every operating room and PACU should have an apparatus for assessing neoromuscular blockade ( and know how to use it !) • TOF, preferably quantitative, monitoring of the neuromuscular block is mandatory if antagonists are not used!! • TOF >0.9 the new ”gold standard” for full recovery Viby-Mogensen. Postoperative residual curarization and evidence-based anaesthesia. BJA 2000
Postoperative pain • a complication itself ? • aggressive pain prophylaxis in all patients Note! • pain must be in proportion to the operative procedure performed • operative/postoperative complication in development • tolerance to opioids
Postoperative pain • discomfort • agitation • PONV • sympathetic activation • cardiovascular complications • hypertension • surgical bleeding • immobilisation • deep vein thrombosis • pulmonary dysfunction • chronic postsurgical pain
Opioid related side effects • PONV • drowsiness • respiratory depression • dysphoria/agitation • gastrointestinal and bladder dysfunction
Balanced or multimodal analgesia • Non-steroidal anti-inflammatory analgesics (NSAIDs) • Paracetamol • Local anesthetics • wound infiltration /neural blockade • liposome local anesthetics in the future? • Combined with • PCA • Epidural
Cyclooxygenase-2 inhibitors in postoperative pain management. Currest evidence and future directionsGilron et al. Anesthesiology 2003
Efficacy of postoperative epidural analgesia. A meta analysisBlock et al JAMA 2003 • 1404 articles in PubMed reviewed of which 1304 rejected • Inclusion criteria • randomization • epidural analgesia versus parenteral opioids in adults • VAS/Numeric rating
Efficacy of postoperative epidural analgesia ; pain at rest Block et al. JAMA 2003
Efficacy of postoperative epidural analgesia; incident pain Block et al. JAMA 2003
Efficacy of postoperative epidural analgesia; VAS recordings Conclusion: Epidural analgesia (other than TEA with opioids only) provides better postoperative analgesia to parenteral opioid Block et al. JAMA 2003
Efficacy of postoperative epidural analgesia; complications Block et al. JAMA 2003
The ”Little big problem of anesthesia”Postoperative nausea and vomiting (PONV) • Patient-specific risk factors • Female sex IA • Nonsmoking status IVA • History of PONV/Motion sickness IVA • Anesthetic risk factors • Use of volatile anesthetics IA • Nitrous oxide IIA • Use of intraoperative IIA and postoperative opioids IVA • Surgical risk factors • Duration of surgery IVA • Type of surgery (laparoscopy, ear-nose-throat, neurosurgery, breast, strabismus, laparotomy, plastic IVB Consensus guidelines for managing postoperative nausea and vomiting Gan et al. Anesth Analg 2003
Postoperative nausea and vomiting (PONV)Keep the baseline risk low ! • Regional anesthesia IIIA • Propofol for induction and maintenence IA • Intraoperative supplemental oxygen IIIB • Adequate hydration IIIA • Avoid nitrous oxide IIA • Avoid volatile anesthetics IA • Minimize intraoperative IIA and postoperative IVA opioids • Minimization of neostigmine IIA Gan et al. Anesth Analg 2003
Algorithm for prevention of PONV Gan et al. Anesth Analg 2003 Multimodal or balanced antiemetic strategy
Prophylaxis of PONVAntiemetic doses and timing in adults Gan et al. Anesth Analg 2003
Treatment of PONV in PACU Gan et al. Anesth Analg 2003
Perioperative mild hypothermia (34-35C);Complications Sessler.Perioperative hypothermia. NEJM 1997
Perioperative maintenance of normothermia reduces the incidence of morbid cardiac events: A randomized clinical trial. Frank et al. JAMA 1997
Perioperative hypothermia and PACU • cardiovascular complications • symphathetic overactivity • norepinephrine • coagulapathy • platelet function • clotting factor enzyme function • fibrinolytic activity • shivering • increased total-body oxygen consumption • patient discomfort • residual neuromuscular blockade • respiratory complications • aspiration • prolongation of PACU stay
Perioperative hypothermia First stage • internal transfer of core heat to periphery i.e., internal redistribution Second stage • drop in core temperature as the result of heat losses • cutaneous, • exposure of viscera • cold solutions Third stage • cutaneous vasocontriction • core temperature remains almost stable but the heat content of the limbs continues to fall • Mild hypothermia 34-35 C Sessler Anesthesiology 2001
Perioperative mild hypothermiaDelay in recovery Lenhard et al.Mild intraoperative hypothermia prolongs postoperative recivery Anesthesiology 2001