Download
1 / 16
210 likes | 2.4k Views
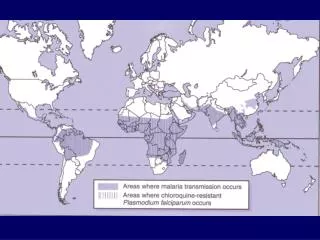
Malaria: Epidemiology Four species: P. falciparum, P. vivax, P. ovale, P. malariae Majority of cases are P. falciparum or P. vivax Most deaths caused by falciparum; predominates in tropical Africa, SE Asia, Haiti, Amazon basin, Dominican Republic

E N D
Malaria: Epidemiology • Four species: P. falciparum, P. vivax, P. ovale, P. malariae • Majority of cases are P. falciparum or P. vivax • Most deaths caused by falciparum; predominates in tropical Africa, SE Asia, Haiti, Amazon basin, Dominican Republic • Vivax most prevalent in Central America, Middle East, India
Life Cycle • Bite of the Female Anopheles mosquito • Sporozoites enter the bloodstream and travel to liver • Divide into mature tissue schizonts, containing thousands of daughter merozoites. (exoerythrocytic stage) • These rupture after 6-16 days and release merozoites into the bloodstream, where they invade RBC’s (erythrocytic stage)
Life Cycle • Within RBC matures from ring form to trophozoites to mature red cell schizonts (vivax, ovale, falciparum = 48 hours, falciparum = 72 hours); this is the asexual form. • Mature schizonts released from RBCs and can infect new red cells. • A few merozoites will differentiate into male or female gametocytes (the sexual form.)
Life cycle • Gametocytes do nothing but circulate in the bloodstream until they are ingested again by a mosquito to complete their life cycle in the gut of the Anopheles. • Vivax and ovale can remain dormant in the liver as hypnozoites and cause late relapse; falciparum and malariae have no dormant phase.
Pathogenesis • All malaria spp. digest red cell proteins and hemoglobin. They derive energy by anaerobic glycolysis; therefore patients are prone to hypoglycemia and lactic acidosis. • Parasites also deform the RBC membrane, causing hemolysis and accelerated splenic clearance. • Thrombocytopenia can occur due to increased splenic sequestration. • Release of proinflammatory cytokines during RBC lysis causes fever, chills, malaise.
Pathogenesis • P. falciparum causes additional pathology by forming sticky knobs on the surface of RBCs via an interaction with actin and spectrin. • Knobs bind to receptors on endothelial cells causing microvascular pathology and occlusion
Clinical manifestations • Fevers/chills that are cyclical • Sweats, headache, myalgias, fatigue, nausea, vomiting, abd pain, diarrhea, cough • Hepatosplenomegaly, jaundice, anemia • Vivax, ovale = invade young RBC’s, low level parasitemia, can have late relapse • Malariae = preferentially invades mature RBCs resulting in low grade parasitemia, mild symptoms • Falciparum = invades all ages RBCs
Complications • Renal failure: due to hypovolemia, microvascular occlusion, hemolysis • Pulmonary: sequestration of infected RBCs in the lung can cause pulmonary edema/ARDS • Hypoglycemia • Anemia, DIC • Splenic rupture
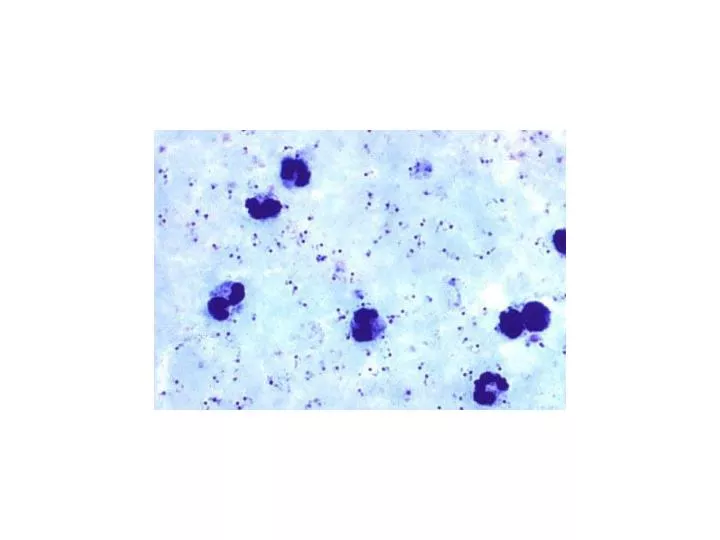
Diagnosis • Travel history • Thick and thin smears: every 6 to 12 hours for 48 hours • Fluorescent microscopy • PCR • Antigen detection
Treatment • Outpatient vs. inpatient • Supportive: antipyretics, glucose containing IVF • No drug acts on all stages of the life cycle • Quinoline derivatives: inhibit heme polymerase activity resulting in accumulation of free heme which is toxic to parasites. Chlorouqine, quinine, quinidine, mefloquine (intra-RBC); primaquine (intra-erythrocytic, intrahepatic, and gametocytes)
Treatment • Antifolates (pyrimethamine, sulfonadmies, dapsone): kill intrahepatic forms (except hypnozoites) , gametocytes • Artemisinin derivatives: not available in the U.S. Bind iron, produce free radicals that damage parasites. • Antimicrobials: clinda, atovaquone, tetracycline—act synergistically to kill blood schizonts
Resistance • Chloroquine: ovale, malariae = not observed. Falciparum = widespread with exception of Haiti, Mexico, Dominican Republic. Vivax = mainly Papua New Guinea • Primaquine: vivax from Thailand • Quinoline: falciparum from SE Asia • Antifolate resistance: prevalent in falciparum throughout the Amazone basin, SE Asia
Treatment • Chloroquine (primaquine if vivax or ovale) or quinine plus antimicrobial for synergy • Parasitemia >5% = iv quinine • Exchange transfusion • Desferrioxamine