Download
1 / 35
420 likes | 579 Views
Glucose Tolerance Test. Dinaz Lahewala Fall 2011. Outline. Background information Class experiment In-depth mechanisms Q & A. Background Info. Glucose: monosaccharide primary source of energy for the brain, muscles, and other essential cells

E N D
Glucose Tolerance Test DinazLahewala Fall 2011
Outline Background information Class experiment In-depth mechanisms Q & A
Background Info • Glucose: monosaccharide • primary source of energy for the brain, muscles, and other essential cells • Important source of energy for cellular processes • Plasma [glucose] is mainly monitor by islets of Langerhans located in Pancreas • Also regulated by actions of different hormones: growth hormones, Epi, Cortisol, & ACTH
Endocrine Pancreas • Human pancreas contains 500,000 to several million islets • Islet of Langerhans • Alpha cells produce glucagon • Beta cells produce insulin • Delta cells produce somatostatin
Insulin • Main regulator of blood glucose • Maintains concentration of glucose in the plasma within narrow limits • Help in the transport of glucose from the blood into other tissues of the body • For metabolism • Storage
Effect of insulin Insulin causes cells in the liver, muscle, and fat tissue to take up glucose from the blood, storing it as glycogen in the liver and muscle, and stopping use of fat as an energy source When control of insulin levels fails => diabetes
Control of Insulin Secretion • Substrate • High blood glucose => release of insulin • Low blood glucose => inhibit release of insulin • Humoral • Gastric inhibitory peptide, glucagon => release of insulin • somatostatin=> inhibit release of insulin • Neural • Ach release by vagalnerve (PSN) => trigger beta cells to release insulin • Epi & NE (SNS)
Feeding period Glucose and neural and GI hormones stimulate beta cells to secrete more insulin Insulin promotes glucose uptake by cells for metabolism, glycogen synthesis, and fatty acid synthesis, etc
Fasting Period: • Low blood glucose level Beta cells secrete lessinsulin • Extended period of fasting/starving: • Pancreas alpha cell is stimulated to secrete glucagon effect liver cells act to increase blood glucose by increased glycogenolysis & gluconeogenesis • Glyconolysis= glycogen converted to glucose • Gluconeogenesis = making of glucose from non-carbohydrate carbon substrate (aa)
Plasma [glucose] • Normal plasma [glucose] is ranging from • 60-140 mg/dl depending on individual dietary intake of glucose, and period of fasting/feeding • Renal threshold for plasma [glucose] is ~ 180 mg/dl • Hypoglycemia: decrease in level of blood glucose (caused by excess of insulin) • Hyperglycemia: excess accumulation of glucose in blood, causes plasma [glucose] level rise from 120-160 mg/dl to as high as 300 mg/dl
Diabetes • Blood [glucose] following glucose ingestion in a normal and diabetic person are different • Normal person: • blood glucose level rises from about 90 mg/dl to around 140 mg/dl in 1 hr, and then falls back to normal (or below normal) within 3 hours due to excess insulin release by pancreas • Diabetic person: • shows hyperglycemic response in which blood glucose level rises to as high as 300 mg/dl and then slowly falls to fasting diabetic level after 5-6 hrs.
Symptoms of diabetes • Hyperglycemia: • Glucouria: urinary excretion of glucose • Result when kidney unable to reabsorb all the glucose • Polyuria: abnormally large vol. of urine • sugar remains in urine an retains water w/in • Polydipsia: Increased water intake • Ketouria: acetone in urine
Diabetic acidosis • When insulin is low • Cells cannot metabolize glucose for energy Inc metabolism of fats and protein Intermediate product of fats breakdown is ketone bodies (e.g acetone) • Ketone bodies => acidic • Drop in blood pH => acidotic • Odor of acetone in urine
Diabetes Mellitus • Type 1 (IDDM): Insulin-dependent diabetes mellitus • Lack of insulin caused by • Viral destruction of beta cells • Chemically induced – alloxan (inhibitors of B cells) • Treatment: insulin injection; pancreas transplant • If not treated acidosis and dehydration could lead to death.
Type 2 –NIDDM Non-Insulin Dependent Diabetes Mellitus • Beta cells present but body is resistant to insulin • Hypotension, obesity. Doesn’t develop severe ketoacidosis • Treatment: take drugs to restore insulin sensitivity
Hormones that raise plasma [glucose] • Suppress glucagon release from alpha-cells • Suppress release of insulin, pituitary tropic hormone, gastrin and secretin • Epinephrine (adrenal medulla): • Enhance release of glucose from glycogen • Enhance release of fatty acids from adipose tissue.
Hormones that raise plasma [glucose] • Cortisol(adrenal cortex) • Enhance gluconeogenesis • Antagonizes insulin • ACTH (anterior pituitary) • Adrenocorticotropic hormone • Enhance release of cortisol • Enhance release of fatty acids from adipose
Hormones that raise plasma [glucose] • Growth Hormone: • Released by Ant. Pituitary • Increases plasma [glucose] by inhibiting glucose transport into the cells ---------------------------------------------------------------- • Somatostatin: • Released from D cells of the pancreas • Inhibits Growth hormone, insulin, glucagon, gastrin, CCK, and reduces GI contractility
Class Experiment • Glucose Tolerance Test: measure the ability of the body (pancreas) to respond to excess ingestion of glucose. • Procedure: • 2 individuals • 1 drink sugar solution (fasted ~12 hours) • 1 drink water • Atevery 30min. interval for 2 hours • Collect blood [glucose] • Check for glucose in urine
Insulin Mechanism Glucose triggers insulin in 7 steps Glucose enters the beta cell through GLUT4* (glucose transporter) by facilitated diffusion in presence of glucokinase, glucose undergoes glycolysis and raises [ATP]i by phosphorylating ADP Increased [ATP]icauses potassium ATP channels to close reducing potassium conductance leads to the depolarization of the beta cell the depolarization activates voltage-gated calcium channels increased calcium permeability gives an increase in calcium influx and an increase in free intracellular calcium increase in [Ca²]ileads to insulin release
Epinephrine Mechanism Secreted by adrenal medulla in response to stimulation by the central nervous system Increase in blood glucose concentration Hormone boosts supply of oxygen and glucose to the brain and muscles Elevates the blood sugar level by increasing catabolism of glycogen to glucose in the liver, and at the same time begins the breakdown of lipids in fat cells Increase Glycogenolysis in muscle increase lipolysis in adipose
Glucagon Mechanism • Glucagon binds to glucagon receptor, a G protein-coupled receptor located in the plasma membrane conformation change in receptor activates G proteins, heterotrimeric protein α, β, γ subunits • When G protein interacts with receptor it undergoes a conformational change that results in the GDP molecule, that was bound to the α subunit, to be replaced with a GTP molecule • Subsitution results in the releasing of the α subunit from the beta and y subunit. Α subunit specifically activates adenylatecyclase • Adenylatecyclase makes cAMP which activates protein kinase A • This enzyme activates phosphorylatekinase which in turn phosphorylates glycogen phosphorylase, converting the active form called phosphorylase A • Phosphorylase A is the enzyme responsible for the release of glucose-1-phosphate from glycogen polymers • Increase Blood Glucose Increase Gluconeogenesis + Glycogeneolysis
Growth hormone Mechanism • Actions oppose the normal effects of insulin • Over secretion of GH causes insulin resistance and often also causes glucose intolerance • It causes release of insulin-like growth factor 1 (IGF-1) • When the GH level is high so is IGF-1 • IGF-1 leads to body growth and effects almost everysingle cell in the body • In Growth Hormone: Increase in calcium & sodium retention Increase Gluconeogenesis Decrease in liver uptake of glucose, which in turn stimulates somatomedin release from liver Increase glucose & amino acids uptake in bone & skeletal muscle Increase in protein synthesis Increase in lipolysis
Cortisol Mechanism • It is involved in response to stress • Controlled by CRH (corticotropin-releasing hormone) • Highest levels present in the early morning • Counteracts insulin, by contributing to hyperglycemia by stimulus of hepatic gluconeogenesis and inhibition of the peripheral utilization of glucose by decreasing the translocation of glucose transporters to the cell membrane especially GLUT4 • Increase Blood glucose Increase Gluconeogenesis + lipolysis
Now its your turn to talk! … or zone back in because its Questions time!
Q/A Q1) How are the levels of insulin and glucagon regulated in the body? A) Negative feedback: When blood glucose is dangerously low => pancreatic alpha cells release glucagon => glycogenolysis => raise blood glucose levels When blood glucose level is high => pancreatic beta-cells release insulin => transport glucose across cellular membrane => lower blood glucose
Q2) What causes the “insulin shock” seen when an overdose of insulin is given to an organism? • A2) Overdose of insulin => more glucose transport to cells => blood glucose falls to very low level => deprives neurons and brain cells a source of energy => interrupted activity tremors, convulsions, weakness,insulin shock
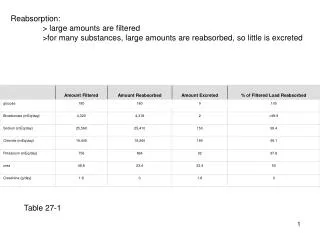
Q3) Why is there an increase in urine output (diuresis) in diabetes mellitus? • A3) Inc. osmolarity of urine • high concentration glucose in blood causes the PCT active transport saturated => max reabsorption is reached => excess glucose falls into urine and pull water with it.
Q) why does a person who has diabetes mellitus have more acidic urine? • A) Intermediate product of fat breakdown is ketone bodies (e.g. acetone) => acidic => lower body pH => acetone release in urine => odor of acetone in urine
Q) some diabetics control their blood glucose level by ingesting tablets rather than receiving injection of insulin. How do tablets work, and who may use them? • A) tablet work improving sensitivity of body's tissues to action of insulin. • For type 2 diabetes