Download
1 / 27

E N D
1. Biliary Pancreatitis Bryan Thompson
April 26, 2004
Gastroenterology Grand Rounds
2. Study #1 Neoptolemos et al United Kingdom
1983 to 1987
Single center
All pts with amylase > 1000 IU/ml and pain typical for pancreatitis had abdominal u/s and �biochemical prediction of gallstones� within 24 hours of admission
3. Study #1 Neoptolemos et al Disease severity predicted by modified Glasgow criteria
Mild attack 0-2 of the following, severe attack > 3 of the following:
Age > 55 years
WBC > 15
Glucose > 180 mg/dL
BUN > 45 mg/dL
PaO2 < 60 mm Hg
Albumin < 3.2 mg/dL
Calcium < 8 mg/dL
LDH > 600 IU/L
4. Study #1 Neoptolemos et al Pts �suspected� of having gallstones were stratified by predicted severity
Exclusion criteria: pregnancy, < 18 y.o., h/o EtOH abuse or acute intake, other identifiable cause of pancreatitis
Cholangitis and elevated bilirubin were not exclusion criteria
Randomized
ERCP + ES within 72 hours of admission
Conservative therapy
All ERCPs performed by a single, skilled endoscopist
After day 5, all pts offered ERCP + ES if felt indicated
No ERCPs in conservative arm prior to day 5
5. Study #1 Neoptolemos et al Outcomes
Local Complications: pseudocysts, ascites, duodenal obstruction
Systemic Complications: respiratory failure, pleural effusion, pneumonia, cardiovascular failure, renal failure, DIC, CVA, death
Cholangitis and sepsis not listed as outcomes
6. Study #1 Neoptolemos et al
7. Study #1 Neoptolemos et al
8. Study #1 Neoptolemos et al 6 pts in ERCP arm and 5 in Conservative arm had cholangitis
If these pts were excluded:
Overall complication rate was 11% with ERCP and 33% with conservative therapy (p = 0.02)
Overall complication rate in predicted severe pancreatitis was 15% with ERCP and 60% with conservative therapy (P = 0.003)
9. Study #1 Neoptolemos et al Length of Hospitalization (days)
10. Study #1 Neoptolemos et al Statistically significant decrease in morbidity and length of hospitalization with ERCP in pts predicted to have severe pancreatitis
Trend towards improvement in mortality but not statistically significant
ERCP is safe in acute pancreatitis
Successful in 80% of pts
Only complication was lumbar osteitis
11. Study #1 Neoptolemos et al Limitations
Pts with cholangitis randomized
No allowance for early ERCP in conservative therapy group, strength or weakness of study?
Mean time to ERCP not mentioned
Single center and endoscopist
12. Study #2 Fan et al Hong Kong
1988-91
Single hospital
All pts with amylase > 1000 IU/ml and pain typical for pancreatitis
Exclusion criteria: prior Billroth II surgery, prior history of non biliary pancreatitis, post ERCP pancreatitis
13. Study #2 Fan et al Randomized
ERCP within 24 hours of admission
Conservative Therapy
ERCP during acute phase for the following:
Rising fever, leukocytosis and tachycardia
Increasing jaundice or serum bilirubin
Shock not responding to IV therapy
ERCP routinely after resolution of pancreatitis
14. Study #2 Fan et al Predicted severity determined by admission BUN and glucose
If glucose > 198 mg/dL or BUN > 45 mg/dL, categorized as severe
Outcomes
Local complications: pancreatic abscess, pseudocyst, phlegmon, and bleeding pseudoaneursym
Systemic complications: renal failure, respiratory failure, cardiogenic shock, bleeding gastric erosions, and DIC
Biliary sepsis: acute cholangitis or cholecystitis
15. Study #2 Fan et al 64% of pts in ERCP group and 63% in Conservative group had biliary pancreatitis
87 of 97 pts in ERCP group had successful ERCP
27 pts in Conservative group required early ERCP, successful in 25 of 27
10 for cholangitis
10 for sepsis
7 for organ failure
16. Study #2 Fan et al
17. Study #2 Fan et al
18. Study #2 Fan et al If only patients with biliary pancreatitis are included
19. Study #2 Fan et al Statistically significant decrease in biliary sepsis in pts predicted to have severe pancreatitis in ERCP group
Statistically significant decrease in morbidity with ERCP in pts with biliary pancreatitis
Trend towards improvement in mortality but not statistically significant
20. Study #2 Fan et al Limitations
Included all causes of pancreatitis
Less commonly used means of predicting severity of pancreatitis
Length of hospitalization not analyzed
21. Study #3 Folsch et al Germany
1989 to 1994
Multicenter
Biliary pancreatitis
Gallstones on ultrasound or CT or
2 of the following 3 laboratory abnormalities
Alkaline phosphatase > 125 U/L
Alanine aminotransferase > 75 U/L
Bilirubin > 2.3 mg/dL
22. Study #3 Folsch et al Exclusion criteria included bilirubin > 5 mg/dL
Randomized to ERCP within 72 hours of symptom onset or conservative therapy
ERCP in conservative group for temp > 102.2o F, increase in bilirubin > 3 mg/dL within 5 days, or persistent biliary cramps
Severity predicted by modified Glasgow criteria
23. Study #3 Folsch et al ERCP Group
ERCP successful in 121(96%) of 126 pts
46% had choledocholithiasis
2 pts had bleeding following sphincterotomy, 1 required PRBC transfusion
Otherwise no direct complications related to ERCP
Conservative Group
22 of 112 pts had ERCP within 3 wks of symptom onset
8 for increasing bilirubin, 8 for elevated temperature, and 6 for persistent biliary cramps
ERCP successful in 19
24. Study #3 Folsch et al
25. Study #3 Folsch et al Study terminated early as increased deaths with ERCP made it highly unlikely that superiority of ERCP would be shown
Conclusion: ERCP not beneficial in acute biliary pancreatitis without biliary obstruction or sepsis
Results unaffected by classifying pts based on predicted disease severity
26. Study #3 Folsch et al Study criticized because many centers only contributed 2 � 3 pts and it was theorized that these centers probably did not have �expert� endoscopists
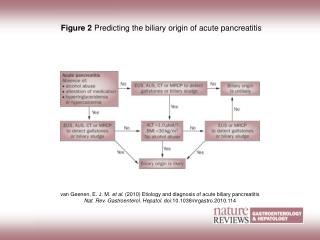
27. Suggested Approach