Download
1 / 32
320 likes | 405 Views
Recruitment of low-income and minority subjects for clinical research . George T. O’Connor, MD, MS Pulmonary Center, BUSM October 7, 2008. Why focus research on inner-city communities?. High-risk, vulnerable population Asthma, diabetes, HTN, HIV, etc.

E N D
Recruitment of low-income and minority subjects for clinical research George T. O’Connor, MD, MS Pulmonary Center, BUSM October 7, 2008
Why focus research on inner-city communities? • High-risk, vulnerable population • Asthma, diabetes, HTN, HIV, etc. • Violence, smoking, environment, addiction, etc. • Socioeconomic and racial disparities, environmental justice • Pathogenetic clues from racial differences • Research funding • Targeted initiatives of NIH and foundations • Major strength of BUMC. This is who we are!
Case studies at BUMC • Framingham Omni Cohort (1994-1999) • Inner-City Asthma Study (1998-99) • Feasability of Retinoid Therapy for Emphysema (2001-2002) • Asthma Genetics Study (2001-2006 ) • Asthma Control Evaluation Study (2004-2006) • Urban Environment and Childhood Asthma Study (Jan 2005 ) • Inner-City Asthma Treatment with Anti-IgE (ICATA) Study (October 2006 ) • Airway Response to Tobacco Smoke (ARTS) Study (2008 )
Barriers to recruiting and retainingresearch participants in low-income urban communities • Can’t be bothered (like everyone else!) – no incentive to participate • Suspicion of investigators • Fear of adverse medical and social consequences of participation • Education • Language and culture • Transportation • Scheduling (too busy vs. too disorganized) • Overly broad exclusion criteria
General approach to recruitment and retention • Investigate best sources of subjects, and be willing to revise plans as needed • Create incentives to participate • Overcome barriers (really…not sort of) • Create relationships • With subjects • With staff who can offer help with recruitment
FHS Omni Cohort • Rationale: We needed minority subjects to qualify for NIH funding! • Demographics: Framingham, MA had changed but FHS had not. • Challenge: Population-based recruitment of minority population of Framingham.
FHS Omni Cohort • Strategy: • Previously recruited 100-member Framingham Minority Cohort • English and Spanish in local newspapers • Church and social groups • Flyers in public places • Direct mailing to all 4914 households intwo Framingham Census tracts with large minority populations • Word of mouth • Subject motivation: Health screening
Men Women Black non-Hispanic 71 113 Hispanic 79 124 Asian / Pac Island 62 56 Native American 2 * White non-Hispanic 3 3 Total 215 298 FHS Omni Cohort
FHS Omni Cohort • Follow-up • 299 of the 500 participated in Sleep Heart Health Study, along with 699 Offspring • Omni: 48 dropped out or lost by 9-10 years • Majority Latino immigrants • Offspring: 5 dropped out or lost by 9-10 years • Limitations • Not as “population-based” as original FHS cohort • Recent immigrants not as stable for long-term follow-up
Inner-City Asthma Study Seattle/Tacoma J. Stout Boston G. O’Connor Bronx E. Crain Chicago R. Evans New York M. Kattan DCC-Chapel Hill H. Mitchell Tucson W. Morgan Dallas R. Gruchalla
ICAS: Study Design • Multi-center, randomized, controlled trial of physician feedback and environmental remediation in seven inner-city environments • 2 x 2 design powered for both interventions • One year of intervention followed by one year of observation
ICAS: Study Population • Children aged 5 to 12 with moderate asthma enrolled from inner-city census tracts (> 20% of families with income below federal poverty level) • Severity in last 6 months: • One overnight hospitalization for asthma - or - • Two unscheduled clinic visits for asthma • Positive skin test to > 1 indoor allergen • Sleep at one address > 5 nights per week
ICAS recruitment issues in Boston • Advantages • BMC provided lists of patients with ER visits or hospitalizations for asthma. IRB allowed us to write parents then call them • Challenges • Patients of Co-PI Suzanne Steinbach, MD excluded (lots of them!) • Compared to other ICAS cities, Boston has well-developed NHC network, free-care system, and asthma specialists available to inner-city children not so many really sick kids • Boston’s inner city smaller than New York, Chicago, etc.
ICAS recruitment history in Boston • Boston always lagged other sites, vying with Seattle for last • Direct contact of patients identified from BMC lists remained most productive source of participants, but it wasn’t enough. • We added: • Census tracts in Lynn, MA, screening at LCHC • Collaborator at Children’s Hospital to identify children from that site • Outreach to staff at HealthNet NHCs • Ads in neighborhood newspapers
ICAS – Lessons learned • Follow recruitment weekly if it’s not working, change it ASAP • Remove transport barriers: we paid for round-trip taxi for GCRC visits • Financial compensation for participants a (the?) major motivating factor! Should reflect fair value of their time and effort. • $50 for coming to GCRC • $10 for home visit • $10 for each two phone call • Intervention groups kept vacuum cleaner, HEPA filter, etc.
Feasability of Retinoid Therapy for Emphysema (2001-2002) • Rat model: all-trans retinoic acid appears to reverse elastase-induced emphysema • NHLBI workshop: recommended studies to examine feasability of human studies • FORTE Study established after RFP and competitive application process • BU, U Pittsburgh, Columbia, UCLA, UCSD
FORTE recruitment • Goal: 60 subjects with emphysema at each site • Age > 44; not currently smoking; not currently on prednisone; etc. • Diffusing capacity < 80% predicted; etc. • > 10% of lung with emphysema by quantitative CT analysis (UCLA CT reading center) • Recruitment proved difficult at all sites (144/300) • Bronchoscopy was part of protocol • Smoking and prednisone were common issues • Medication exclusions included calcium channel blockers
FORTE recruitment at BUMC • The birth of HIPAA: No access to BMC lists of patients with COPD, emphysema • Alternative: BMC sends list of own patients with diagnosis to PCP PCP sends to us list of those OK to contact We write letter from PI and PCP to patient We get PCP to sign letter, then we mail it Follow-up phone call to patient. • IRB approved this, but we never pulled it off
FORTE recruitment at BUMC • Minority recruitment goals: • I initially proposed 30% in my application • I later reduced this to 10% when NHLBI pressed us for realistic numbers • We recruited no minorities at BUMC • WBZ ad calls • Boston radio station with African-American audience no calls • My own patients no interest • Typical BUMC participants: White, internet-connected patients from Maine to Florida • Study-wide: 1 minority subject of 144 total
FORTE – Lessons learned • You may not be able to recruit minority subjects for a given study in proportion to the demographics seen at BMC. • ? African-American patients especially reluctant to consider experimental medications and invasive procedures
Asthma Genetics Study • Initial hypothesis focuses on IL-16 promoter polymorphism • 400 asthmatics and 200 non-asthmatic controls with goal of about 2/3 African-American and Latino • Phone screen: Age < 44, smoking < 10 pack-years • Single visit of about 1 hour: questionnaires, spirometry, blood draw. $30 compensation.
Asthma Genetics Study • Identification and recruitment of asthmatics • Our own patients: • High yield but numbers limited • Letter then phone call from research team • Referral from pulmonary and PCC colleagues • They have to think of it!.. And they won’t • Ads: Metro paper works well, although milder asthma severity and fewer minorities
Asthma Genetics Study • Identification and recruitment of controls • Genetic association studies and population stratification • Initial plan: friend control of same gender and similar age and racial-ethnic background • Most cases not providing friend control • When they do, racial-ethnic match is very good • Revised plans: • Added $10 “finder’s fee” compensation for referral • Open up to non-referred control volunteers, collecting detail info on race and ethnicity • Hang out in Ortho Clinic to recruit health controls: not efficient
Research recruitment in Boston’s low-income communities: lessons learned • Ethnic background and linguistic abilities of research staff should match target population. • Plan on recruitment being the most difficult challenge of the study, and have the staff to devote the needed time. • Making a separate trip to BUMC is a big barrier. • Use multiple recruitment modalities as needed. • Compensate participants fairly. • Be ready to revise plans as you go. • Depending on the study, it might not work!
Hi Tom, An issue that has bothered me for some time is the following. Our IRB here at BUMC prohibits us from mentioning in flyers and advertisements the dollar amount of compensation that participants in clinical research will receive. I guess the rationale for this policy is that listing $ amounts will somehow be coercive. This policy seems misguided to me for several reasons: 1. Most other institutions permit advertising dollar amounts. Any day of the week you will see ads from the Brigham offering specified dollar amounts to research volunteers. 2. The IRB will, quite appropriately, not let an investigator pay a coercive amount. Instead, we offer reasonable compensation for time and effort. 3. If we want the ad or flyer to provide adequate info on which a prospective volunteer can base a decision whether it is worth his/her time to call about the study, listing the dollar amount would be beneficial to the volunteer. 4. It will greatly help us recruit subjects. Can we change the BUMC policy on this? Thanks for your consideration of this issue. George
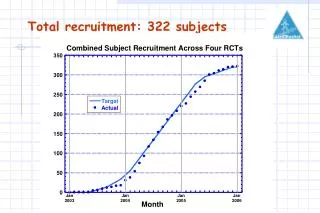
Two more recent studies of Inner-City Asthma Consortium… • Asthma Control Evaluation (ACE) Study • 320 (52 Boston) asthmatics age 12-20 • RCT of eNO in asthma management • 9 visits over 1 year; $815 compensation plus transportation (we arranged and paid for taxis) • Urban Environment and Childhood Asthma (URECA) Study • 500 (125 Boston) newborns with parental history of asthma or allergy • Birth-cohort study (recruit pregnant women) of environmental risk factors for asthma • 3 years follow-up in initial phase; home and clinic visits; $495 compensation plus transportation
Two more recent studies of Inner-City Asthma Consortium… • Asthma Control Evaluation (ACE) Study • Sources of subjects: Dr. Steinbach’s practice; some referrals from NHCs or school nurses; newspaper ads • Motivating factors: $815; both groups received frequent specialist asthma care • Urban Environment and Childhood Asthma (URECA) Study • Sources of subjects: Prenatal practice at BMC. • Key to success: Aviva-Lee Parritz, MD as co-investigator • Motivating factors: $495; interest in whether child will develop asthma and allergy
Airway Response to Tobacco Smoke (ARTS) Study • Never, former, current, and passive smokers • Single visit with nasal and oral mucosa brushing and blood mRNA arrays, along with spirometry and questionnaire. • $50 compensation for one-hour visit • BU “Quickie Jobs,” Craigslist, Metro ads not many heavy smokers; no passive smokers • Soliciting smokers in front of Menino Pavilion and at BUMC bus stops whoa, baby!!
Community involvement in research • A “holy grail” that I have yet to really figure out how to apply. • Focus of some NIEHS RFAs • Who exactly is “the community” and how “involved” should they be in our research? • Models involving churches, etc. • Colleagues at JHU in Baltimore: community advisory board for their research on inner-city asthma (Swartz LJ et al., Methods and issues in conducting a community-based environmental randomized trial. Environ Res. 2004; 95:156-65.) • Project ACCESS in Boston – in progress
Acknowledgments • The incredibly talented and hard-working study coordinators and research assistants who make it all possible • Carolina Jordan, MPH; Lisa Gagalis, RN; Martine Dumas, MPH • IRB staff