Download
1 / 29
290 likes | 374 Views
Of Mothers, Orphans and the HIV Pandemic. Karen P. Beckerman, MD Associate Professor of Obstetrics and Gynecology New York University Director of Obstetrics Bellevue Hospital Center 25 October 2002. New slides needed: CSx data: 367, 316, Models of HIV Rx in dev world

E N D
Of Mothers, Orphans and the HIV Pandemic Karen P. Beckerman, MD Associate Professor of Obstetrics and Gynecology New York University Director of Obstetrics Bellevue Hospital Center 25 October 2002 New slides needed: CSx data: 367, 316, Models of HIV Rx in dev world Tb Rx and dev world Ask Ester if she might consider a picture of herself and her daughter Rupert and his son.
HIV disease in the U.S. Pediatric AIDS incidence Reproductive Health and HIV Principles of care: universal developed world Preconceptional and early pregnancy counseling Vertical Transmission Principles of care during pregnancy The global epidemic
December 2001: • > 40 million infected • >8,000 deaths per day • 600 new infections per hour • a child dies every minuteOctober 2002: • 5 million new infections in 2001 • 800,000 children infected • 44 million orphans by 2010
Reproductive Health & HIV • Pregnancy does not alter the course of HIV disease in the west. • Data do not exist examining the effect of pregnancy on HIV progression in the developing world. • Prospective studies show that a pregnant HIV infected mother has a 3% chance dying before her baby’s first birthday and an 11% chance of dying before the second birthday.
HIV in Africa • DATA are VERY SCARCE ! • The epidemic is heterosexual. • After infection, rapid progress to AIDS. • Less than half will remain symptom-free at 3 years. • Median survival is 9 years. • Survival with AIDS is “short.”
HIV and African Women • 55% of infected individuals are women. • Male to female transmission is 10x more efficient that female to male. • Women are infected early in their reproductive lives, • Ususally by older men. • Rates of pregnancy and nursing are high among African women with asymptomatic HIV.
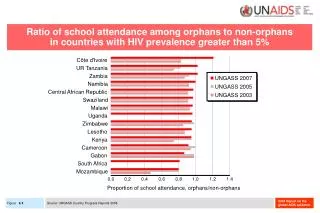
“The Population Chimney” • HIV mortality will produce population pyramids that have never been seen before. • By 2010, men will outnumber women in each 5-year cohort between 15 and 49. USAID, “Children on the Brink”
Largescale orphaning: • Historically, sporadic and short term. HIV orphaning: • Long term and chronic. • Will worsen in coming decades. • Most will be uninfected. • All will face extraordinary risks: Inadequate nutrition, housing and health care. Servitude, harshness & abuse Acquisition of HIV
Proposed Solutions to the Orphan Crisis: • Strengthen coping capacities of families • Protection of property and inheritance rights • District AIDS committees • Community day-care centres • Waiving school fees • Support youth expression • Encourage political will • Reduction of stigma • Promote the rights of women and children • Encourage partnership and leadership-USAID, 2001
Principles of care of the HIV-1 infected pregnant motherFirst things first: • Safe shelter • Adequate nutrition • Transportation • Self-determination
Self Determination: Reproductive choice OI Prophylaxis Treatment Delivery plan
Principles of care of the HIV-1 infected pregnant motherProtection of mothers from mono- and dual therapies likely to induce ART resistance:
Low Fidelity HIV-1 Replication • Two polymerases without proofreading activity HIV-1 reverse transcriptase Cellular RNA polymerase • Two RNA copies per virion Insertions and deletions are common • RNA strand breaks force template switching • Uracil incorporation into proviral DNA Especially in resting cells
Pregnancy and ART resistance in UgandaNVP single dose prophylaxis: HIVNET 006 & 012Single dose to mother + single dose to infantTransmission fell from 25 to 13% • 10 of 46 mothers studied 6 weeks to 6 months later had detectable resistance • Of the 36 infected infants, 8 had detectable nnRTI resistance at 6 weeks of age.
Principles of care of the HIV-1 infected pregnant motherProtection of mothers from mono- and dual- therapies likely to induce resistance: • Nevirapine prophylaxis (even one dose) is highly likely to result in nnRTI resistance if not given in a safe combination. • In the U.S., nevirapine prophylaxis given in addition to standard ART resulted in no benefit to mother or baby, but did cause significant induction of nnRTI resistance.(Dorenbaum, PACTG 316, CROI, 2001)
Pregnancy and ART resistance in the developed world • Zidovudine/lamivudine (AZT/3TC) induces resistance (M184V) at same frequencies in pregnant women as in men • In one study, 4 of 5 mothers developed M184V (Clark, J Med Virol.59:364) • M184V can be transmitted to neonates
Pregnancy and ART resistance in the U.S. and England: Are these data relevant to us today? Unfortunately, YES.ACTG 185: late 1990s • 86% received ZDV 14% received ZDV/3TC • 30% of mothers had nRTI resistance by delivery • These mothers were 3 times more likely to transmit virus to their infant (p=0.03)
Principles of care of the HIV-1 infected pregnant motherProtection of mothers from mono- and dual- therapies likely to induce resistance: • Women refusing 3 medications should be offered zidovudine prophylaxis, never Combivir alone. Combivir Alone
Priniciples of care of the HIV-1 infected pregnant motherAggressive use of combination antiretroviral therapy to achieve durable suppression of maternal HIV replication and to protect mother from induction of antiretroviral resistance: • Offer 3 or more medications • Twice daily dosing