Download
1 / 67
690 likes | 1.48k Views
ANEMIAS. Bone marrow examination. Bone marrow examination refers to the pathologic analysis of samples of bone marrow obtained by bone marrow biopsy (often called a trephine biopsy) and bone marrow aspiration

E N D
ANEMIAS Dr. Alka Stoelinga
Bone marrow examination • Bone marrow examination refers to the pathologic analysis of samples of bone marrow obtained by bone marrow biopsy (often called a trephine biopsy) and bone marrow aspiration • A bone marrow biopsy removes a small amount of bone and a small amount of fluid and cells from the bone • A bone marrow aspiration removes only the marrow. Dr. Alka Stoelinga
Site of procedure • Children <2 years of age: • Medial aspect of upper end of tibia >2 years of age: • Posterior iliac crest • Adult • Mid manubrium sterni • Sternal body • Posterior iliac crest Dr. Alka Stoelinga
Materials required: • Lidocaine cream with occlusive dressing • 16-gauge 2-1/2 or V bone marrow needle • (3) 10ml syringes • 25-gauge needles • 20-gauge needles • 4 x 4 and 2 x 2 gauze pads • Povidone-iodine swabs • Sterile drapes • Lidocaine 1% multidose vial • Alcohol swabs • Elastoplast adhesive, or other pressure dressing • Sterile gloves Dr. Alka Stoelinga
Procedure 1. Prior to the procedure • Obtain consent for procedure. • Notify hematology dept • Determine and obtain appropriate type and dose of sedation and pain medications. Schedule child for anesthesia if elective and child/adolescent have no contraindications for anesthesia. Instruct patient/family in NPO requirements. Prepare the patient for the procedure: a. Explain the basic steps of the procedure, appropriate for the patient's age, development status, and prior experience. b. Encourage the parent's/patient’s participation, answering all questions honestly given the available knowledge. c. Explain that while parts of the procedure are painful, the use of a local anesthetic and sedation medications will minimize the discomfort and anxiety the child will experience. d. Elicit the patient's help by encouraging them to hold as still as possible once positioned. Reinforce the patient's help in holding still will enable you to complete the procedure in the minimum amount of time. e. During the procedure, explain each step in a simple manner, preparing the patient for painful parts of the BMA. Dr. Alka Stoelinga
Procedure 2.Apply Lidocaine cream 1-2 hours prior to the procedure 3. At the time of the procedure: • Wash hands. • Assemble supplies and medications, checking expiration date on BMA tray. • Administer sedation medications, monitoring vital signs, pulse oximetry, level of sedation. • Remove outer wrapping from bone marrow tray using clean technique. • Position patient in prone or side-lying position. Dr. Alka Stoelinga
Procedure • Expose area for aspiration and locate posterior superior iliac crest. • Remove Lidocaine from aspirate site. A towel roll or small pillow placed under the hips may allow easier location of the iliac crest. • Position the parent near the child's head in order to more easily comfort the child during the procedure. • Expose contents of bone marrow tray using aseptic technique. • Put on sterile gloves. • Swab bone marrow site with Povidone-iodine swab stick, applying some friction and working in a circular motion beginning in the center and moving outward. Repeat x 2 with new swabs. • Allow povidone-iodine to dry. • Remove povidone-iodine with alcohol swab using concentric motion beginning in the center. Repeat with new swab x 2 (optional). • Allow area to dry. • Apply sterile drape. • Draw up 2-3ml lidocaine 1% from a vial held by an assistant into a 3 ml syringe with a 22 gauge 1 " needle. • Locate exact point for aspiration and outline area between thumb and index finger. • Perpendicularly inject lidocaine subcutaneously upto periosteum. Dr. Alka Stoelinga
Procedure 4. While allowing 2-3 minutes for lidocaine to take effect: • Prepare bone marrow needle, assuring stylet moves freely. • Prepare (2) 10ml syringes, assuring plungers move freely. Remove top from one syringe and set aside. Prepare second syringe (if needed for special studies) using 0.2ml heparin and rinsing inside of syringe. Set aside. • Stretch skin taunt over puncture site, keeping crest between thumb and index finger of one hand. • Holding bone marrow needle with stylet in place, puncture skin and advance through subcutaneous tissue, periosteum and into marrow cavity using a steady, controlled pressure with a twisting motion. When the needle is firmly in place and a slight give in pressure is felt, the cavity has been entered. • Remove the stylet and quickly attach the plain syringe to the needle hub. • Apply strong, quick suction and obtain approximately 0.5ml marrow. • Hand syringe to the lab technician/ assistant. • Obtain other samples with heparinized syringe as needed. • Remove needle with syringe attached with slight twisting motion. Dr. Alka Stoelinga
Procedure • Maintain pressure over site approximately 2 minutes until bleeding has stopped. • Meanwhile, remove sterile drape and cleanse povidone-iodine from skin with alcohol swab to avoid burn. • Apply dry 2x2 gauze folded into quarters and secured with tightly stretched Elastoplast. • Praise the patient's cooperation. • Inform patients / parents and child of marrow result when obtained. BM BIOPSY • A trephine needle is inserted and anchored in the bony cortex. • The needle is then advanced with a twisting motion and rotated to obtain a solid piece of bone marrow. • This piece is then removed along with the needle 5. Patient conditions requiring consultation: • Unusual bleeding, pain or signs/symptoms of concern to the practitioner will be brought to the attention of the responsible fellow or attending physician. • After two unsuccessful attempts, a fellow, attending will complete the procedure. Dr. Alka Stoelinga
Procedure 6. After the procedure • After the procedure is complete, the patient is typically asked to lie flat for 5–10 minutes to provide pressure over the procedure site. • After that, assuming no bleeding is observed, the patient can get up and go about their normal activities. • Paracetamol (acetaminophen) or other simple analgesics can be used to ease soreness, which is common for 2–3 days after the procedure. • Any worsening pain, redness, fever, bleeding or swelling may suggest a complication. • Patients are also advised to avoid washing the procedure site for at least 24 hours after the procedure is completed Dr. Alka Stoelinga
The aspirate yields semi-liquid bone marrow, which can be examined by a pathologist under a light microscope and analyzed by flow cytometry, chromosome analysis, or polymerase chain reaction (PCR). • Frequently, a trephine biopsy is also obtained, which yields a narrow, cylindrically shaped solid piece of bone marrow, 2mm wide and 2 cm long (60 μL), which is examined microscopically (sometimes with the aid of immunohistochemistry) for • Cellularity and infiltrative processes • An aspiration, using a 20 mL syringe, yields approximately 300 μL of bone marrow. • A volume greater than 300 μL is not recommended, since it may dilute the sample with peripheral blood Dr. Alka Stoelinga
Causes of Dry Tap • Aplastic anemia • Myelofibrosis • Hairy cell leukaemia • Multiple myeloma • Metastatic carcinoma • Faulty technique Dr. Alka Stoelinga
Iron deficiency anemia Dr. Alka Stoelinga
Iron deficiency anemia • Anemia due to iron losses or physiological requirement exceeding absorption • Dietary intake or absorption of iron is insufficient • Hemoglobin cannot be formed Dr. Alka Stoelinga
AETIOLOGY • Reproductive age- Female: • Menorrhagia • Gastrointestinal bleeding • Pregnancy • Pathological blood loss • Deficient diet • Parasitic infestations- Hookworm • Adult Male+ Postmenopausal women: • Pathological blood loss • Malabsorption • Inadequate diet • Parasitic infestations- Hookworm • Children and infants • Deficient diet • Deficient iron stores at birth • Parasitic infestations- Hookworm Dr. Alka Stoelinga
CLINICAL FEATURES Symptoms • Tiredness • Lightheadedness • Breathlessness • Dizziness/ Tinnitus/ Headache/ Dimness of vision • Ankle swelling • Worsening of any previous coexisting disease- Angina • Pica- Eating items like Coal, soil etc Signs • Pallorness of Mucous membrane + Skin • Tachypnea/ Exertional dyspnea • Raised JVP • Flow murmurs • Ankle edema • Postural hypotension • Tachycardia • Koilonychia • Angular stomatitis • Glossitis • Dysphagia due to formation of esophageal webs (Plummer-vinson syndrome). • Restless leg syndrome • Pruritis Dr. Alka Stoelinga
INVESTIGATIONS • Hb- Reduced • Peripheral blood film: • Microcytic hypochromic anemia • Anisopoikilocytosis- Target cells, Pencil cells, Tear drop cells • RBC Indices (MCV, MCH, MCHC)- Reduced • Biochemical: • Serum Ferritin level- Reduced (Specific) • Serum Iron, Saturation of iron: Reduced • TIBC, RDW- Increased • Bone marrow: • Erythroid hyperplasia, Micro-normoblastic erythropoiesis, no stainable iron • Others: • Stool for Routine and Occult blood test, barium meal X-ray, Upper and Lower GI endoscopy Dr. Alka Stoelinga
Rx • Ferrous sulphate 200mg TID/ 8hrly for 3-6 months • Ferrous gluconate 300 mg 12 hrly • Hb should rise by 1g/dl every 7-10 days • Failure to respond • Non Compliance • Continued blood loss • Malabsorption • Incorrect diagnosis • Malabsorption • Inj. Fe sorbitol (1.5 mg of iron/ kg body wt) Intramuscular • Iron dextran iv or im at 3 months Dr. Alka Stoelinga
Effect of vitamin and mineral supplements • There is an observed correlation between serum retinol and hemoglobin levels. • Women with a low serum retinol concentration are more likely to be iron-deficient and anemic, compared to those with normal to high levels of retinol. • Vitamin A deficiency has an adverse effect on hemoglobin synthesis, even a slight increase in vitamin A intake can lead to a significant rise in hemoglobin levels • However, vitamin A is less effective in alleviating severe iron-deficiency anemia. • Low levels of iron in the body cannot be relieved by vitamin A supplementation alone. • Additionally, a low ascorbic acid stores in the body causes an impairment in the release of stored iron in the reticuloendothelial cells. • Copper is necessary for iron uptake, and a copper deficiency can result in iron deficiency. • Copper deficiency can sometimes be caused by excessive zinc or vitamin C supplementation. Dr. Alka Stoelinga
MEGALOBLASTIC ANEMIA Dr. Alka Stoelinga
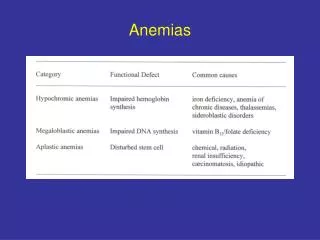
MEGALOBLASTIC ANEMIA • Megaloblastic anemia is characterized by presence of erythroblasts in bone marrow with delayed maturation due to defective DNA synthesis. • Anemia due to deficiency of Vit B12 or Folic acid Dr. Alka Stoelinga
Vitamin B12 deficiency alone will not cause the syndrome in the presence of sufficient folate • The mechanism is • Loss of B12 dependent folate recycling • Followed by folate-deficiency loss of nucleic acid synthesis (specifically thymine) • Leading to defects in DNA synthesis • When DNA synthesis is impaired, the cell cycle cannot progress from the G2 growth stage to the mitosis (M) stage • This leads to continuing cell growth without division, which presents as Macrocytosis Dr. Alka Stoelinga
Megaloblastic anemia not due to hypovitaminosis may be caused by antimetabolites that affects DNA production directly, such as some chemotherapeutic or antimicrobial agents (for example azathioprine or trimethoprim). • It is characterized by • Many large immature and dysfunctional red blood cells (megaloblasts) in the bone marrowand • Hypersegmented or multisegmented neutrophils Dr. Alka Stoelinga
Causes • Vitamin B12 deficiency leading to folate deficiency: • Achlorhydria-induced malabsorption • Deficient intake • Deficient intrinsic factor (pernicious anemia or gastrectomy) • Coeliac Disease • Biological competition for B12 by diverticulosis, fistula, intestinal anastomosis, and infection by the marine parasite Diphyllobothrium latum (fish tapeworm) • Selective B12 malabsorption (congenital and drug-induced) • Chronic pancreatitis • Ileal resection and bypass • Nitrous oxide anesthesia (usually requires repeated instances) • Folate deficiency: • alcoholism • Deficient intake • Increased needs: pregnancy, infant, rapid cellular proliferation, and cirrhosis • Malabsorption (congenital and drug-induced) • Intestinal and jejunal resection • (indirect) Deficient thiamine and factors (e.g., enzymes) responsible for folate metabolism. • Combined Deficiency: Vitamin B12 & folate. • Inherited Pyrimidine Synthesis Disorders: Orotic aciduria • Inherited DNA Synthesis Disorders • Toxins and Drugs: • Folic acid antagonists (Methotrexate) • Purine synthesis antagonists (6-mercaptopurine) • Pyrimidine antagonists (cytosine arabinoside) • Phenytoin • Nitrous Oxide • Erythroleukemia Dr. Alka Stoelinga
CLINICAL FEATURES Dr. Alka Stoelinga
INVESTIGATIONS • The blood film: • Decreased red blood cell (RBC) count and hemoglobin levels • Increased mean corpuscular volume (MCV, >95 fl) and mean corpuscular hemoglobin (MCH) • Normal mean corpuscular hemoglobin concentration (MCHC, 32–36 g/dL) • The reticulocyte count is decreased due to destruction of fragile and abnormal Megaloblastic erythroid precursor. • The platelet count may be reduced • Neutrophil granulocytes may show multisegmented nuclei ("senile neutrophil"). • This is thought to be due to decreased production and a compensatory prolonged lifespan for circulating neutrophils, which increase numbers of nuclear segments with age. • Anisocytosis and poikilocytosis • Macrocytes • Ovalocytes • Howell-Jolly bodies (chromosomal remnant) also present. • Blood chemistries will also show: • Increased lactic acid dehydrogenase (LDH) level. • The isozyme is LDH-2 which is typical of the serum and hematopoietic cells. • Increased homocysteine and methylmalonic acid in B12 deficiency • Increased homocysteine in folic deficiency • Normal levels of both methylmalonic acid and total homocysteine rule out clinically significant cobalamin deficiency with virtual certainty. • Bone marrow shows Megaloblastic hyperplasia. Dr. Alka Stoelinga
The gold standard for the diagnosis of B12 deficiency is a low blood level of B12. • A measurement of methylmalonic acid can provide an indirect method for partially differentiating B12 and folate deficiencies. • The level of methylmalonic acid is not elevated in folic acid deficiency. • Direct measurement of blood cobalamin is the gold standard because the test for elevated methylmalonic acid is not specific enough. Dr. Alka Stoelinga
Pernicious anemia • Autoimmune disorder in which gastric mucosa is atrophied with loss of parietal cells causing intrinsic factor deficiency leading to Vit B12 deficiency • Intrinsic factor is necessary for absorption of dietary Vit B12 • Common in people aged 40-60 • With Family H/O Pernicious anemia or auto immune diseases like Hashimoto’s thyroiditis, Grave’s disease, Vitiligo, Hypoparathyroidism or Addison’s disease Investigations • Antiparietal cell antibody • Antibodies to Intrinsic factor in serum Diagnostic Dr. Alka Stoelinga
Folate deficiency Sources • Leafy vegetables- Spinach, broccoli, lettuce • Fruits- Bananas, melons • Animal proteins- Liver, kidney Dr. Alka Stoelinga
Treatment Vit B12 deficiency • Hydroxycobalamine 1000 micrograms i.m in 5 divided doses 2-3 days F/B Maintenance therapy • 1000 micrograms every 3 monthly for life Folate Deficiency • Oral folic acid 5mg daily for 3 weeks f/b maintenance therapy • 5mg once weekly Dr. Alka Stoelinga
Hemolysis Dr. Alka Stoelinga
Hemolysis Dr. Alka Stoelinga
Intravascular hemolysis • Rapid cell destruction • Free Hb released in plasma • Haptoglobin produced by liver • Binds with free Hb and is degraded in liver • Once Haptoglobins (Are reduced) are saturated, • Free Hb is oxidised • Methemoglobin + Albumin • Methemalbumin- degraded • Any Free Hb is bound to Haemopexin • If all of these mechanisms are saturated/ overloaded, Free Hb urine • When fulminant black urine (Falci. malaria) • In smaller amt Renal tubular cells absorb Hb, degrade it and store iron as hemosiderin • Subsequently tubular cells- sloughed- urine- hemosideriuria Dr. Alka Stoelinga
Extravascular hemolysis • Physiological Red cell destruction in RE cells in liver, spleen • Haptoglobulins are normal or slightly reduced Dr. Alka Stoelinga
Features of Hemolysis Blood film Spherocytosis No Spherocytosis Fragmentation • Hereditary • Enzymopathies DCT+ DCT- • Microangiopathic • Traumatic • Autoimmune hemolysis • Malaria • Clostridium • H. spherocytosis Dr. Alka Stoelinga
Congenital hemolysis • RBC membrane defects (hereditary spherocytosis/ Elliptocytosis) • G6PD deficiency • Hemoglobinopathies Dr. Alka Stoelinga
Red cell membrane defect • Defect in cytoskeleton • Usually due to quantitative or functional deficiency of one or more proteins in cytoskeleton • Cells loose their normal elasticity • Each time they pass through spleen, they lose membrane relative to their cell volume Raised MCHC Abnormal shape Reduced cell survival (EVH) Dr. Alka Stoelinga
Hereditary Spherocytosis • Autosomal dominant trait • 25% have no family history • Abnormalities in Beta spectrin and ankyrin Hemolytic crisis- when severity of hemolysis increases Megaloblastic crisis- follows folate deficiency Aplastic crisis- Parvovirus infection • Presents with severe anemia and low reticulocyte counts Dr. Alka Stoelinga
Investigations • Blood picture- presence of spherocytes • DCT –ve • Osmotic fragility test- Increased sensitivity to lysis in hypotonic saline solution Treatment • Folic acid prophylaxis 5mg once weekly • Blood transfusion after cross matching • Consider splenectomy • Growth retardation in children • Recurrent severe crisis • Death of a family member from the disease • Symptomatic cholecystitis Dr. Alka Stoelinga
G6PD deficiency • HMP shunt • NADPH – protects red cells against oxidative stress • G6PD deficiency Impairs production of NADPH • Affects male; females are carriers Clinical Features: • Acute drug induced hemolysis • Chronic compensated hemolysis • Infection or acute illnesses • Neonatal jaundice • Favism (Vicia fava/ broad beans) Dr. Alka Stoelinga
Investigations • Evidence of nonspherocytic intravascular hemolysis • Bite cells, blister cells, irregular small cells • Polychromasia reflecting reticulocytosis • If stained with methyl violet- denaturated Hb is visible as Heinz bodies within RBC cytoplasm • G6PD levels- low Treatment • Stop precipitating drugs • Acute transfusion support- life saver Dr. Alka Stoelinga
Autoimmune Hemolytic Anemia • Red cell autoantibodies RBC destruction • IgG/ M, rarely IgE or A CLASSIFICATION • Optimal temperature at which the antibody is active is used to classify AHA • 1. Warm antibodies • bind best at 37⁰C • Majority are IgG • React against Rh antigens • 80% of cases • 2. Cold antibodies • Bind best at 4⁰C but can bind upto 37⁰C • Majority are IgM and bind compliment • 20% of cases Dr. Alka Stoelinga