Download
1 / 19
190 likes | 265 Views
Family-level clustering of childhood mortality risk in Kenya . D. Walter Rasugu Omariba Department of Sociology Population Studies Centre University of Western Ontario London, Ontario. Background. Mortality decline in Kenya began in late 1940s.

E N D
Family-level clustering of childhoodmortality risk in Kenya D. Walter Rasugu Omariba Department of Sociology Population Studies Centre University of Western Ontario London, Ontario
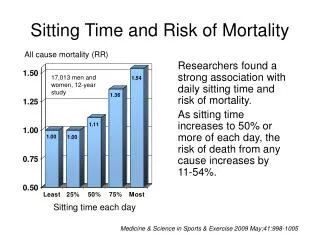
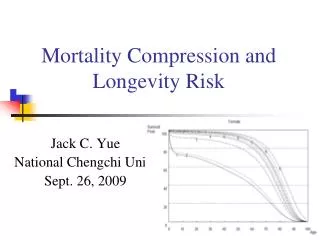
Background • Mortality decline in Kenya began in late 1940s. • E.g. under-five mortality: 220 in 1958-62 period, declined to 89 in 1984-1989 period • Reversals in the downward trend started in 1986 (see figure 1). • Infant mortality increased by 24 % and • Under-five mortality by 25 % in 1988-98 period.
Figure 1: Child mortality trends 1974-1998, Kenya Source: National Council for Population and Development and Macro International, 1989, 1994; 1999.
Focuses on determinants and differentials of mortality (See, for instance, Kibet, 1981; Ewbank et al., 1986; Kichamu, 1986; Omariba, 1993; Obungu et al., 1994; Ikamari, 2000). This study’s focus: Familial child death clustering: In the literature, defined in two ways: 1) Expected vs. observed- Higher observed deaths indicate death clustering 2) Control for unobserved heterogeneity through inclusion of random effects in models- correlation of risks at different levels. Existing research
Rationale • Random-effects models used yet to be applied on Kenyan data. • Child mortality remains an important public health issue. • Reducing mortality important for sustaining country’s incipient fertility transition.
Sources of unobserved heterogeneity • Differential competence in childcare (Das Gupta, 1997). • Biological factors e.g. genetically determined frailty, ‘improvident maternity’ syndrome (Guo, 1993; Das Gupta, 1997). • Socioeconomic, cultural factors and environmental factors. • All unmeasured and unmeasurable factors.
Death clustering? • In this study: • Measured by unobserved heterogeneity term indicating correlation of risks in family. • Most studies only select one child, truncate data by certain date or ignore first child- Biased results especially when variables such as preceding birth interval and survival status are considered.
Implications of data structure • Children in same family are more alike than children from different families. • covariates’ estimates biased. • Consequences of violation of independence: • standard errors of parameters underestimated– spurious precision. • biases baseline hazard duration pattern downward in survival analysis.
Implications of data structure • Random-effects models: Correct for the biases in parameter estimates, provides correct standard errors and correct confidence intervals and significance tests • Separates impact of individual and social context • If contextual effects significant, using a random effect (or multilevel model is reasonable). If not, then we need only adjust the error term for dependence of units.
Data and methods • Data source: Demographic and Health Survey for Kenya, 1998. • 7,881 women 15-49, all marital statuses from 8,380 households and 8,233 eligible women. • 3,407 husbands/partners of the women • Largely rural sample, 81.4% of the women’s sample • Methods: • Weibull hazard models and random-effect hazard models. • The latter tests for family-level variance.
Conceptual framework • Study is guided by the Mosley and Chen (1984) ‘proximate determinants’ model (see Figure 2). • Individual characteristics: Migration status, education, year of birth, ethnicity, religion, survival status of preceding child, birth interval, birth order and maternal age at birth. • Household characteristics: socioeconomic status, sanitation and source of water.
Figure 2:Conceptual framework for studying the determinants of infant and childhood mortality Proximate Determinants Distant Factors -Reproductive healthcare behaviour e.g. prenatal care, place of delivery, delivery care, tetanus injection, breastfeeding -Biodemographic factors e.g. maternal age at birth, birth interval, birth order, age at marriage, child loss experience -Household environmental conditions e.g. source of water, toilet facility. -Socio-economic factors: e.g. maternal & paternal education, place of residence, region, migration, occupation, household socioeconomic status, marital status, year of birth, period of child birth. -Socio-cultural factors: e.g. religion, ethnicity. Outcome Variable Risk of child death
Data description: • Of the 7881, 5716 had at least one child, while 2165 had never had a child. • 23348 children born to 5716 women (family) • 2325 children had died before their fifth birthday: • Infancy- 1620(0-12 months) • Childhood- 705 (Age 13-59 months)
Table 3: Distribution of children and child deaths per family in Kenya, DHS 1998
Does clustering exists? • Over 80 percent of the children belong to families contributing two or more children to the sample. • Families with six or more children comprise about 28 percent of the families yet contribute over half of the children. • 57 percent of the deaths occurred to 8.6 percent of the families with two or more deaths. • About 2 percent of the families contribute four or more deaths; together accounting for about 18 percent of the deaths.
Results • There is significant unobserved heterogeneity both in infancy and childhood (Tables 3 &4): • The estimated random parameters, θ, in the models with unobserved heterogeneity are 0.40 and 0.78 for infant and child mortality respectively. • There is significant familial variation in the risk of infant and child death. • Maternal education, period of birth, ethnicity, type of toilet facility, birth interval and maternal age at birth of child important for both infant and child survival (Tables 1&2). • Migration status, religion, survival status of previous child and birth order significant only for infant mortality, while household SES significant only for child mortality.
Results • There are large ethnic differences in risk of death with children Luo mothers being most disadvantaged. • Secondary or higher education associated with a 22 % and 42% reduction in risk of infant mortality and child mortality respectively. • Risk of infant death higher for children born after 1990, while that of child death is higher for all children born after 1985. • The risk of infant death is higher for children whose sibling died, were born less than 19 months after preceding sibling, and when the mother was less than 20.
Conclusions • The determinants of death have different effects on infant and childhood mortality. Biodemographic factors have greater effect in infancy, while education and ethnicity have greater effect in childhood. • Suggests varied policy actions: • Infancy: longer birth intervals through family planning and breastfeeding, later age at birth etc. • Childhood: improvement in education, socioeconomic status and poverty eradication programs.
Conclusions • Death clustering is non-ignorable – Needs further research: • Healthcare factors- Information available only for children born three years before the survey. • Qualitative research at community level. • Death clustering, another measurement: Consider unobserved heterogeneity in the context of each woman’s sequence of births. The heterogeneity term used in this paper does not reflect this fact.