Download
1 / 111
1.11k likes | 1.28k Views
Prion Diseases. Kuru. Kuru figures. Incidence 1 % (population aprox. 15,000) total F : M = 10 : 1 < 20 years of age F : M = 3 : 1 (20 % of cases) 20-40 years of age F : M = 15 : 1. Etiology of Kuru. Primary infectious: no fever, no CSF cell raise Genetical disease:

E N D
Kuru figures • Incidence 1 % (population aprox. 15,000) total F : M = 10 : 1 • < 20 years of age F : M = 3 : 1 (20 % of cases) • 20-40 years of age F : M = 15 : 1
Etiology of Kuru • Primary infectious: no fever, no CSF cell raise • Genetical disease: • Pro: in families, in patients who moved out of Fore region. • Con: also in patients who came to live in Fore region, as well in young as in old patients. • Toxic/deficiency: no toxic compound isolated, balanced diet. • Endocanibalism
Sporadic CJD 1920/1921
Sporadic Creutzfeldt-Jakob disease diagnosis • Rare disease: 1/106 • Duration: short (months) • Neurological signs and symptoms: Rapidly progressive dementia, myoclonus, ataxia, central visual disturbances, extrapyramidal signs, pyramidal signs, akinetic mutism (variant: chorea, dysesthesias, psychiatric disturbances) • EEG and MRI • Neuropathology • WHO criteria: • Type of CJD (sporadic, genetic, iatrogenic, variant) • Strength of diagnosis (definite, probable, possible)
MRI EEG abnormalities normal sCJD Weighted T2 Proton density
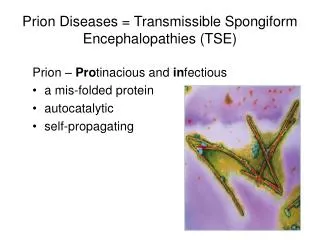
Prion Diseases/Transmissible Spongiform Encephalopathies Prion diseases TSE's in animals TSE's in man sporadic 85% Scrapie sCJD }14% genetic fCJD ex-Scr acq. by infection GSS CWD FFI TME }1% Kuru BSE iCJD FSE vCJD ex-TSE
Etiology • Possibilities (ca 1980): • Degenerative/Hereditary • (slow)Virus
Againts virus hypothesis • Very resistant agent: • resists dry heat ( > 200ºC) • resists steam autoclaving (up to134ºC, 18 mins.) • resists formaldehyde • resists UV-radiation • resists Gamma-radiation ( > 0.3 MGray) • etc.
Prion docterine (Prusiner) • In biochemical separation-infection studies: • Infectivity is not present in a DNA/RNA fraction • Infectivity is present in a protein fraction • In conclusion: • A protein (and that protein only) causes a prion disease
51 1 22 91 codon 219 231 254 129 -8 polymorph. E/K M/V α3 ß1 α1 ß2 α2 PRNP 5 OR sign. peptide Glycin - prolin rich sequency hydrophob. seq. CHO α3 α3 ß1 ß1 α1 α1 ß2 ß2 α2 α2 PrPc/PrPSc (33 - 35 kD) 5 OR CHO CHO GPI Proteinase K CHO S S S PrPSc (27- 30 kD) CHO GPI PrPc-fragm. S S S From Prion gene to Prion protein
Octa-repeat H1 H3 N-terminus GPI H2 Sh1 Sh2 129 106-126 PrPC
PrPC to PrPSc Abnormal folding of a protein protein (and that protein only) causes a prion disease
Polymerisation Dimerisation PrPSc PrP* PrP* PrP* PrPSc PrPC PrP* PrPSc PrPSc PrPC PrPSc PrPSc Conversion models for PrPC to PrPSc …and subsequent breaking and seeding.