Download
1 / 16
170 likes | 443 Views
NICE Guidelines on Recognition and Assessment of Coeliac Disease (May 2009). Sarah Jane Rapsey ST2 . Coeliac Disease. Genetically-determined chronic inflammatory disorder of the small intestine. Increased immune response to gluten, a protein found in wheat, rye, barley, (oats).

E N D
NICE Guidelines on Recognition and Assessment of Coeliac Disease (May 2009) Sarah Jane Rapsey ST2
Coeliac Disease • Genetically-determined chronic inflammatory disorder of the small intestine. • Increased immune response to gluten, a protein found in wheat, rye, barley, (oats). • Often co-exists with other conditions. • Prevalence: 1% in UK. • 4.5-12% risk if 1st degree relative affected
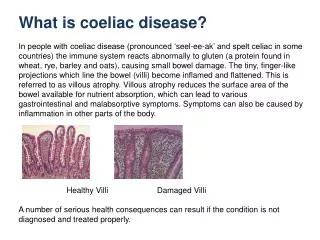
Pathophysiology • Sensitivity to gliadin (alcohol-soluble protein component) in gluten. • Genetic link: HLA DQ2 locus (90%) • Small intestinal mucosa accumulates sensitised Tcells- cytokine release. • Flattening of villi resulting in malabsorption of nutrients.
Presentation of Coeliac Disease • May present at any age after weaning. • Children: malabsorption; diarrhoea, weight loss, failure to thrive. • Adults; anaemia (folate/iron deficient), abdo discomfort, bloating, diarrhoea, steatorrhoea, fatigue, malaise.
Complications of Coeliac Disease • Malabsorption of iron, folic acid, vitamin B12, calcium, vitamin D, vitamin K. • Lactose intolerance. • Osteoporosis, increased risk of fracture. • Pregnancy complications; IUGR, preterm labour. • Intestinal malignancy; NHL, HL, small bowel ca. • IgA deficiency in 2% of coeliacs.
Dermatitis Herpetiformis • Skin manifestation of coeliac disease. • Raised, red patches, often blistered. • Commonly on elbows/knees/buttocks. • Symmetrical • Skin biopsy, treated with dapsone.
Testing for Coeliac Disease • Serology: • Anti-tissue transglutaminase antibodies (TTG)-involved in destruction of villous extracellular matrix and villous epithelium. • Endomysial antibodies • Small intestinal biopsy=gold standard.
NICE Guidelines 2009; Recognition and Assessment of Coeliac Disease
Conditions: Autoimmune thyroid disease. Dermatitis herpetiformis IBS Type 1 diabetes 1st degree relative with coeliac disease Signs and Symptoms Chronic or intermittent diarrhoea Persistent/unexplained GI sxms Recurrent abdo pain/distension Failure to thrive in children Unexplained iron def anaemia Tired all the time NICE recommends offering serological testing to adults and children with….
GI tract problems Microscopic colitis Persistent unexplained constipation Persistent raised LFTs Aphthous ulceration Autoimmune disorders Autoimmune liver conditions Autoimmune myocarditis Bone disorders Low trauma fracture Reduced bone mineral density Metabolic bone disease Genetic disorders Down’s syndrome Turner’s syndrome Gynae symptoms Amenorrrhoea Recurrent miscarriage Unexplained subfertility Other disorders Addisons disease Chronic thrombocytopenia purpura Depression/Bipolar disorder Epilepsy Lymphoma Polyneuropathy Sarcoidosis Sjogren’s syndrome Unexplained alopecia NICE recommends considering testing in adults and children with...
Pre-test counselling; follow-up biopsy. • Testing (serology/biopsy) can only be done when eating a gluten-containing diet in more than one meal per day for 6 weeks. • Tissue transglutaminase is preferred to endomysial antibodies. EMA useful if TTG equivocal. • Exclude IgA deficiency.
Interpreting results of coeliac serology • If positive: refer to gastro for intestinal biopsy. • If negative but ongoing clinical suspicion, refer for biopsy. • If negative and no other reason to suspect coeliac disease, no need for further testing. • Do not start gluten-free diet until diagnosis confirmed on intestinal biopsy.
Management of Coeliac Disease • Gluten-free diet(products available on Rx) • Primary Care Gastroenterological society recommends: • Annual primary care review: BMI, Bowel function, Bloods;FBC,folate,ferritin,alb,ALP, Vitamins D and B12. • Immunisations. • Osteoporosis monitoring: DEXA scan at diagnosis, repeat at menopause in women and age 55 in men or after any fragility fractures.
Summary • Coeliac disease may present with a variety of symptoms and is associated with many other conditions. • Non-gastroenterological consequences. • Serology does not diagnose coeliac disease but indicates whether further testing is needed. • Gluten-containing diet 6 weeks before testing. • Remember IgA deficiency. • Once diagnosis established, review annually for nutritional status and osteoporosis risk.
References • Coeliac Disease, NICE Clinical Guideline (May 2009); Recognition and Assessment of Coeliac Disease. • The GP Update Handbook-Autumn 2009. Primary Care Education LLP. • The management of adults with coeliac disease in primary care, Primary Care Society for Gastroenterology (May 2006).
NICE Guidelines on Recognition and Assessment of Coeliac Disease (May 2009) Sarah Jane Rapsey ST2