Download
1 / 39
410 likes | 787 Views
Prevention of UTIs: Role of Hormones & Probiotics. 가톨릭 의대 한 창 희. 9 th Catholic Urology Symposium. Outline. Vaginal ecosystem Estrogen and recurrent UTI in women What are probiotics and how do they work? Current proposed uses and a look at some of the evidence

E N D
Prevention of UTIs: Role of Hormones & Probiotics 가톨릭 의대 한 창 희 9th Catholic Urology Symposium
Outline • Vaginal ecosystem • Estrogen and recurrent UTI in women • What are probiotics and how do they work? • Current proposed uses and a look at some of the evidence • Issues in prescribing their use 9th Catholic Urology Symposium
Health vaginal ecosystem • Dynamic Equilibrium exists between: • Epithelium • Normal colonizing organisms (mostly Lactobacilli SPP.) • Local secretory and celluar immune factors • Vaginal pH maintained • acidic (3.8 ~ 4.2) • creates unfavourable environment for pathogen 9th Catholic Urology Symposium
Normal Vaginal flora • LACTOBACILLI • Gram positive rods • Excrete hydrogen peroxide • Present in 100% of women with normal flora • Affects adherence of epithelial cells • Protect against bacterial/candidal infections 9th Catholic Urology Symposium
Facultative organisms • Diphtheriods • Coagolase negative Staphycococci • Streptococci • E. coli • Ureaplasma urealyticum • Mycoplasma hominis 9th Catholic Urology Symposium
Anaerobic organisms Present in low, non-pathogenic concentrations • Peptostreptococus • Bacteroides • Fusobaterium • Mobiluncus • Gardnerella (40% - 60%) in normal secretions 9th Catholic Urology Symposium
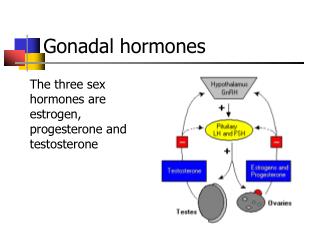
Estrogen; epithelial glycogen • Lactobacilli; glycogen -> lactic acid • Lactic acid maintains acid pH • Abnormal pH (over 4.2) • aggravating factors: • trauma • low estrogen • menses • alkaline seminal fluid • alters vaginal ecosystem • causes epithelial desquamation Lactic acid H2O2 Lactobacillus Glycogen estrogen Normal vaginal flora; protective role 9th Catholic Urology Symposium
UTI in women • 1 billion each year (Reid, 2003) • > 300 million cases annually worldwide (Reid 2001. Am J Clin Nutr 73: S437-S443) • Each episode: on average 6 days of symptoms • Sequelae: pyelonephritis --> preterm birth • Uropathogens: E. coli (approx. 70%), EnterobacteriacaeEnterococcus faecalis, Staphylococcus spp. • Increasing drug resistance among uropathogens 9th Catholic Urology Symposium
Female GU Tract Infections:Disturbance of normal vaginal flora • UTI:Escherichia coli Gram negatives Staphylococcus aureus • BV: "lactobacilli deficiency syndrome" Gardnerella vaginalis, Atopobium vaginae,anaerobes, Mycoplasma hominis, Ureaplasma urealyticum • Yeast vaginitis:Candida albicans 9th Catholic Urology Symposium
Which are the 'right' lactobacilli?Identification of cultured vaginal lactobacilli using tDNA-PCR Verhelst R. et al. BMC Microbiol. 2005, 5: 61 9th Catholic Urology Symposium
Risk factors for BV • The vagina is not a steady state ecosystem. • Menstruation cyclic changes in the vaginal environment • Levels of estrogen and progesterone alter, • Changing the environment for lactobacilli by influencing • cell surface receptor expression • levels of glyocgen and glucose as substrate • levels of vaginal pH • Estrogen protective: • BV prevalence lower in women using oral contraception (Yen et al. 2003) • BV lower during pregnancy (3rd trimester) (Hay et al. 1994) • Clinical trials with estradiol cure of BV, restorationpH, ...(Kanne & Jenny 1991, Parent et al. 1996, Ozkinay et al. 2005) 9th Catholic Urology Symposium
Risk factors for BV • Race/ethnicity (black women at higher risk): • In Africa: > 50% of women have BV (Paxton et al. 1998) • L. iners instead of L. crispatus?(Anukam et al. 2005) • genetic differences in epithelial surface molecules --> different adherence? • Frequency and kind of intercourse: • new male sexual partner • more male sexual partners • female sexual partner • * Sexual intercourse once a week was the only risk factor associated with loss of H2O2 producing lactobacilli. (Vallor et al. 2001) • --> BV is STD? or raise of pH? 9th Catholic Urology Symposium
HSV2 infection (Cherpes TL 2005. CID 40:1422) • HIV shedding (Cu-Uvin S. 2004. CID 33: 894, Sewankambo. 1997. Lancet 350: 546) -->perinatal mother-child HIV-transmission --> sexual HIV-transmission • susceptibility for HIV-infection • infection with CT and HPV (da Silva CS. 2004. GOInvest. 58: 189) • early loss after IVF (Eckert LO. 2003. IDOG 11: 11-17) • associated with recurrent UTI (Hooton TM. 2001. IJAA 17: 259-268) • associated with PID, postpartum endometritis, ... Sequelae of BV (and UTI) 9th Catholic Urology Symposium
Bacterial vaginosis (BV) Number of germs Bacterial vaginosis Normal Lactobacillus Symptoms Gardnerellavaginalis Anaerobes pH 4.0 - 4.5 pH 5.0 - 6.0 9th Catholic Urology Symposium
Estrogens; Clinical trials • A controlled trial of intravaginal estriol in postmenopausal women with recurrent UTIs Raz R, Stamm WE. N Engl J Med 1993, 329:753-756 • 93 postmenopausal women with a history of recurrent UTIs • Randomized, double-blind, placebo-controlled trial of topical intravaginal estriol cream • UTI incidence;0.5 vs. 5.9 episodes per patient-year • Lactobacilli restoration after one month; 61% vs 0% • Vaginal pH declined (from 5.5 to 3.8) • Vaginal Enterobacteriaceae fell from 67 to 31% with estriol but unchanged (from 67 to 63 %) with placebo • prevents recurrent UTI in postmenopausal women, probably by modifying the vaginal flora. 9th Catholic Urology Symposium
World Health Organization: “live microorganisms which when administered in adequate amounts confer a health benefit on the host” A bacterial strain that: survives the stomach acid and bile adheres to intestinal lining grows and establishes temporary residence in the intestines imparts health benefits Probiotics: definitions R Fuller. Probiotics: The Scientific Basis. London: Chapman and Halls. 1992 9th Catholic Urology Symposium
Lactobacillus sp. reuteri casei ramnosus acidophilus Streptococcus sp. Bifidobacterium sp. infantis lactis longum breve bifidum Sacharomyces boulardii (non-human) Probiotics 9th Catholic Urology Symposium
History of Probiotics • Pasteur (1877) • antagonistic interaction between bacterial strains • non-pathogenic bacteria should be used to control pathogenic bacteria • Metchnikoff (1907) • lactic fermentation of milk arrested putrefaction • consumption of fermented products would offer the same benefit to humans • longevity in Bulgarian peasants was due to ingestion of “soured milks” • 1980’s Fuller establishes first definition of probiotics. 9th Catholic Urology Symposium
Probiotics;Potential Mechanisms of Action • Inhibition of adhesion • Immunomodulation • Production of antimicrobial substances • Modification of toxins or toxin receptors • Competition for nutrients • Reduction in bacterial translocation • Anti-inflammatory signaling within the epithelium 9th Catholic Urology Symposium
Infectious diarrhea Antibiotic-associated diarrhea IBD, IBS, and pouchitis Necrotizing Enterocolitis Bacterial vaginosis Recurrent UTI’s Atopic diseases Immune system enhancement H pylori infections Dental caries Radiation induced diarrhea Cardiovascular risk reduction Constipation Rheumatoid arthritis Probiotics: Proposed uses 9th Catholic Urology Symposium
Probiotics: Proposed uses Ratings: A: strong B: good C: fair Floch, et al. Recommendations for Probiotic Use. J Clin Gastro. 40(3). 2006 www.naturalstandard.com 9th Catholic Urology Symposium
Probiotics: Prescribing • Which organism to use? • Which product? • For what conditions? • What dose? • How long? • Any side effects to be aware of? • How much does it cost? 9th Catholic Urology Symposium
Vaginal probiotics; Clinical trials • Treatment of BV with lactobacilli • 60 women with BV • double blind, placebo-controlled trial • Immediately after completion of treatment, • 16/28 women treated with lactobacilli had normal vaginal wet smear results • none of the 29 women treated with placebo. • Only 3of the women who received the Lactobacillus suppository were free of BV after the subsequent menstruation. Hallen A, et al. Sex Transm Dis. 1992, 19:146-148. 9th Catholic Urology Symposium
Vaginal probiotics; Clinical trials • Vaccination against nonspecific BV; Double-blind study of Gynatren • 167 patients with nonspecific BV • vaccinated with Gynatren, a Lactobacillus vaccine • double-blind, randomized, placebo-controlled trial • During the study period of 14 months, vaccination was significantly better than the placebo as concerns its therapeutical effect • Vaccination with Gynatren is effective to prevent recurrences of nonspecific vaginosis. Siboulet A. Gynakol Rundsch. 1991;31(3):153-160 9th Catholic Urology Symposium
Vaginal probiotics; Clinical trials • An audit of Gynatren (a L. acidophilus lyophilisate) vaccination in women with recurrent bacterial vaginosis. Pattman RS et al. Int J STD AIDS. 1994, 5: 299 • Bacterial vaginitis: protection against infection and secretory immunoglobulin levels in the vagina after immunization therapy with Gynatren. Ruttgers H. Gynecol Obstet Invest. 1988, 26: 240-9 • Effect of Lactobacillus immunotherapy on genital infections in women (Solco Trichovac/Gynatren). Karkut G. Geburtshilfe Frauenheilkd. 1984, 44: 311-4 • Randomized double-blind study on the prevention of reinfection intrichomoniasis using Solco Trichovac vaccination.Litschgi M. Gynakol Rundsch. 1982, 22: 70-3 9th Catholic Urology Symposium
Vaginal synbiotics; Clinical trials • Therapy of bacterial vaginosis (BV) using exogenously-applied L. acidophili and a low dose of estriol: a placebo-controlled multicentric clinical trial. Parent D, et al. Arzneimittelforschung. 1996, 46: 68-73 • Vaginal tablets (Gynoflor) containing 50 mg of a lyophilisate of viable, H2O2-producing L. acidophilus(>107 CFU/tablet) and 0.03 mg estriol • 32 non-menopausal women with BV • 6-day therapy with 1~2 vaginal tablets daily • cure rate 2 wks after the start of therapy; 77% vs 25% • cure rate 4 wks after the start of therapy; 88% vs. 22% • A significant increase in the number of lactobacilli 9th Catholic Urology Symposium
Vaginal synbiotics; Clinical trials • The effectiveness of live lactobacilli in combination with low dose estriol (Gynoflor) to restore the vaginal flora after treatment of vaginal infections.Ozkinay E, et al. Brit. J. Obstetr. Gynaecol. 2005, 112: 234-40 • Randomised, placebo-controlled, double-blind clinical trial • 360 women with vaginal infections • Restoration therapy with live lactobacilli in combination with low dose estriol (n = 240) or placebo (n = 120) 2~7 days after the end of the anti-infective therapy • Follow up at 3~7 days and 4~6 weeks after the end of the restoration therapy • Restoration of the vaginal flora can be significantly enhanced by the administration of live lactobacilli in combination with low dose estriol. 9th Catholic Urology Symposium
Non-Vaginal probiotics; Clinical trials with Yoghurt • Ecological treatment of bacterial vaginosis.Chimura T, et al. Jpn J Antibiot. 1995, Mar;48: 432-6 • 11 women with BV: intravaginal application of 5 ml of commercial yoghurt (pH 4.3). • Evaluation after 3 days: vaginal discharge and bacteriology • Significant decrease of vaginal discharge and redness • Vaginal pH was lowered significantly. • Overall bacteriological effects: 6 (54.5%) were eradicated, 3 were partly eradicated, 2 were replaced. • Lactobacillus therapy was effective in both clinical and bacteriological responses. 9th Catholic Urology Symposium
Non-Vaginal probiotics; Clinical trials with Yoghurt • Bacterial vaginosis in pregnancy treated with yoghurt. Neri A, et al. Acta Obstet Gyecol Scand 1993, 72: 17-22 • 32 women with BV in the first trimester of pregnancy were treated with intravaginal application of yoghurt. • The result was favorable. • Ingestion of yogurt containing Lactobacillus acidophilus as prophylaxis for candidal vaginitis. Hilton E, et al. Ann Intern Med 1992, 116: 353-7 • Daily ingestion of 8 ounces of yogurt containing L. acidophilusdecreased both candidal colonization and infection. 9th Catholic Urology Symposium
Non-Vaginal probiotics; Clinical trials • Augmentation of antimicrobial MDZ therapy of BV with oral probiotic L. rhamnosus GR-1 and L. reuteri RC-14: randomized, double-blind, placebo controlled trial. Anukam K, et al. Microbes Infect. 2006 • 125 premenopausal women with BV • Oral MDZ (500 mg) bid for 7 d + oral L. rhamnosus GR-1 (1x109)and L. reuteri RC-14 (1x109) or placebo bid for 30 d • Cure rate of BV; 88% vs 40% (p < 0.001). • Recovery of Lactobacillus sp. counts (> 105 cfu/ml) 96% vs 53% • Use of lactobacilli and antibiotic in the eradication of BV in black African women is efficacious. 9th Catholic Urology Symposium
Non-Vaginal probiotics; Clinical trials • Oral use of L. rhamnosus GR-1 and L. fermentum RC-14 significantly alters vaginal flora: randomized, placebo- controlled trial in 64 healthy women. Reid G, et al. FEMS Immunol Med Microbiol. 2003, 35: 131-4 • 64 healthy women • Oral capsules of L. rhamnosus GR-1 and L. fermentum RC-14 given daily for 60 days • Restoration from asymptomatic BV microflora to a normal lactobacilli colonized microflora; 37% vs 13% (P=0.02). • A significant increase in vaginal lactobacilli at day 28 and 60 • A significant depletion in yeast at day 28 • A significant reduction in coliforms at day 28, 60 and 90 for lactobacilli-treated subjects 9th Catholic Urology Symposium
Non-Vaginal probiotics; Clinical trials • In vitro testing of Lactobacillus acidophilus NCFM as a possible probiotic for theurogenital probiotic applications. Reid G. Int Dairy J. 2000, 10: 415-9 • Oral probiotics can resolve UTI. Reid G. FEMS Immunol 2001, 30:49-52 • Assessment of the capacity of lactobacilli to inhibit growth of uropathogens. Osset J et al. JID 2001, 183: 485-91 • Probiotic feeding reduces UTI in preterm infants. Dani C et al. Biol Neonate 2002, 82: 103-8 • Probiotics: alternative treatment in urology. Hoesl & Altwein. Eur Urol 2005, 47: 288-96 9th Catholic Urology Symposium
Vaginal probiotic products • CTV-05: L. crispatus 108 cfu/capsule (Chrisope Tech., La & Gynelogix, Colo.) • Fem-Dophilus: L. rhamnosus GR-1™ and L. reuteri RC-14™ (Urex Biotech) • Florajen: L. acidophilus 2 x 1010/capsule (American Lifeline, Wisconsin) • Gy-Na-Tren: L. acidophilus 2 x 109 cfu/capsule (Vitalis, Nederland) • Gynoflor: L. acidophilus 107 cfu + 0.03 mg estriol/tablet (Mithra, Liège, fromGrünenthal, produced by Medinova (Zürich, S) • Infemin: L. crispatus, L. acidophilus, L. fermentum, L. rhamnosus, all at109 cfu/ml (Pierre Fabre Sante, Boulogne, France) • Intrafresh: vaginal probiotic pessarium: PEG + L. acidophilus(BioCare, UK) • Lacto AC: 10 species/capsule. TJCP: The Jordan Prentice Co., Fl. • LactoFem: L. Rhamosus,L. acidophilus both at 109/capsule (Mithra, Belgium) • Trenev Trio (Vitals, Nederland) 9th Catholic Urology Symposium
Vaginal probiotics: Rationale to develop • Clear hypothesis about role of lactobacilli • Clearly established protective role of lactobacilli • Lactobacilli are predominant in the vagina. • Application can be topical reaching high inocula no organoleptic considerations • Easy to perform clinical trials: Easy sampling Easy re-isolation of probiotic lactobacilli after application • Already available 9th Catholic Urology Symposium
Probiotics vs antibiotics • Antibiotics • damage commensal microflora. • can increase the occurrence of resistant bacteria • can have adverse side effects • Probiotics • can be used in adjunction to antibiotics to restore the commensal microflora 9th Catholic Urology Symposium
Probiotics; Practical Issues • Not FDA regulated • Quality control is poor • 80% of preparations tested had 1% or less of the bacterial concentration on the label • Numerous preparations on the market • Which strains work best? • Do different strains work better for different diseases? • Do combinations work better than single strains? • May need several months of therapy to see an effect • Likely stop working after discontinued • Concentration (dose) highly variable 9th Catholic Urology Symposium
Conclusions • The use of probiotics in prevention of UTI is promising. • Should be used carefully and cautiously, and only on the basis of strong scientific evidence. • Response is species specific; the success of one species of Lactobacillus in a certain application does not imply that all related strains of this species will be capable of producing a comparable response. • Carefully conducteddouble-blind, placebo-controlledstudies to document the individual efficacy of each specific organism for each potential clinical application are needed. 9th Catholic Urology Symposium