Download
1 / 61
620 likes | 765 Views
Addressing Teen Substance Use: A Clinical Perspective on Adolescent Brain Development. Ken Winters, Ph.D. Department of Psychiatry University of Minnesota winte001@umn.edu Drug Free Communities – Waukesha County Waukesha, WI September 26, 2013. Resources.

E N D
Addressing Teen Substance Use:A Clinical Perspective onAdolescent Brain Development Ken Winters, Ph.D.Department of PsychiatryUniversity of Minnesotawinte001@umn.edu Drug Free Communities – Waukesha County Waukesha, WI September 26, 2013
Resources Brief Interventions and Brief Therapies for Substance AbuseTIPS #34, SAMHSA-CSAT www.samhsa.gov/csat/csat.htm Enhancing Motivation for Change in Substance Abuse TreatmentTIPS #35, SAMHSA-CSAT www.samhsa.gov/csat/csat.htm MotivationalIinterviewing, Third Edition: Preparing People for Change The Guilford Press (2013) www.guilford.com $
Resources $ $ Adolescents, Alcohol, and Substance Abuse: Reaching Teens through Brief InterventionsThe Guilford Press (2001) www.guilford.com Motivational Interviewing with Adolescents and Young Adults The Guilford Press (2011) www.guilford.com TeenIntervene Hazelden Press (2012, 2nd edition) www.hazelden.org $
Outline of Talk • Brief Interventions (BI) • Screening • Motivational Interviewing (MI) • Teen Intervene Update • Case Example
Outline of Talk • Brief Interventions (BI) • Screening • Motivational Interviewing (MI) • Teen Intervene Update • Case Example
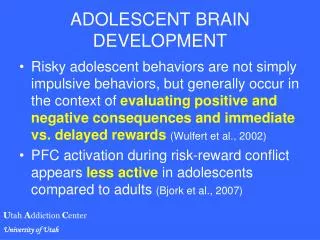
Seven Implications of Arrested Development for Adolescent Behavior • Preference for …. • physical activity • high excitement and low effort activities • activities with peers that trigger high intensity/arousal • novelty • Less than optimal.. • balance of emotion and logic when making decisions • consideration of negative conseq. • Greater tendency to… • take risks and show impulsiveness
Response OptionsAdapted from Broadening the Base of Alcohol Treatment (IOM) Primary Prevention (Intensive for High Risk) MI has several applications within intensive tx Brief Intervention Intensive Treatment Assess & Referral Challenges Dependence Abuse Misuse Infrequent use Drug Involvement Abstinence
Cost Containment Bull Market: 1980’s - mid 1990’s Prevention Tx Gap Intensive Treatment Dependence Abuse Early abuse Infrequent use Drug Involvement Abstinence Adapted from Broadening the Base of Alcohol Treatment (IOM)
Cost Containment Bear Market: since mid 1990’s higher or more stringent admission threshold Brief Intervention- MI Prevention Tx Gap Intensive Treatment Dependence Abuse Misuse Infrequent use Drug Involvement Abstinence Adapted from Broadening the Base of Alcohol Treatment (IOM)
Estimates of Mutually Exclusive “Mild-to-Moderate” Drug Abusing Groups of Youth (12-18-years-old) (based on data from SAMHSA, 2005) 4.4% light drinkers 65.7% non users Total % = 24.7 % Binge and heavy alcohol: past 30 days Abuse only, Illicit drug, and dependence: past year
How Brief is a Brief Intervention? • Some have been a few minutes or a single session (usually during an opportunistic situation). • Typical: 2-4 sessions.
Assumptions of Brief Intervention“Thinking Outside the Box” • Public health, not disease • Harmful consequences on a continuum • Recognize abstinence as ideal but open to alternatives • Does not have to enable addiction Therapy as usual
Why Brief Interventions Makes Sense for Youth • Person-centered approach is appealing to young people. • Commitment to lengthy and intensive interventions can be difficult at this age. • Multiple applications
Possible Applications Brief Intervention Schools, courts, pediatric clinics, emergency rooms, mental health clinics Primary Prevention Intensive Treatment Dependence Abuse Misuse Infrequent use Drug Involvement Abstinence Adapted from Broadening the Base of Alcohol Treatment (IOM)
Cautions • May not be appropriate for severe end cases (e.g., dependence) • Supplemental treatment is warranted to address co-existing conditions • Non-abstinence goals common to brief interventions (e.g., harm reduction, risk reduction) may not be suitable for some settings and for some counselors’ clinical orientation • Abstinence via shaping (“reduction to abstinence”)
Outline of Talk • Brief Interventions (BI) • Screening • Motivational Interviewing (MI) • Teen Intervene Update • Case Example
Screening Issues Primary Prevention (Intensive for High Risk) Brief Intervention Intensive Treatment Screening & Referral Challenges Dependence Abuse Misuse Infrequent use Drug Involvement Abstinence
Screening Issues Primary Prevention (Intensive for High Risk) Brief Intervention Intensive Treatment 1 standardized screening tool & brief clinical interview Screening & Referral Challenges Dependence Abuse Misuse Infrequent use Drug Involvement Abstinence
Screening vs. Assessment Prob Identif. Referral Tx Plan ScreeningProbable? Assess? NA AssessmentDefinitive? Treatment? Goals/Strategy?
My Favorite Screens • Brief screening • CRAFFT • Screening • ADI • DAST-Adolescent • PESQ • SASSI-adolescent • GAIN-Short Screen
Interview - General Issues • Who should be in the room for first session? • maximizing adolescent engagement • consider dividing the session: • both first, then youth alone, OR • youth first, then parent
Brief Interview - HEADS H = Home E = Education/Eating A = Activities D = Drugs S = Sex/Suicidality/Safety
Outline of Talk • Brief Interventions (BI) • Screening • Motivational Interviewing (MI) • Teen Intervene Update • Case Example
Interviewing Techniques Confrontational vs. Motivational
Contrasts Between Confrontational and Motivational ApproachesMiller & Rollnick, 1991 Confrontational Motivational Heavy emphasis on self as having a De-emphasis on labels problem and acceptance of diagnosis Emphasis on personality pathology, Emphasis on personal choice which reduces personal choice and control and responsibility Therapist presents evidence of problems Therapist focuses on eliciting the client’s own concerns
Contrasts Between Confrontational and Motivational ApproachesMiller & Rollnick, 1991 Confrontational Motivational Resistance is seen as “denial” which is Resistance is met with reflection confronted. nonargumentation. Goals of treatment and strategies, Treatment goals and strategies prescribed, client assumed to be are negotiated; clients involvement incapable of sound decisions seen as vital
When is a confrontational style (in light form) indicated? ________________________________________ ________________________________________ ________________________________________ ________________________________________
The Goal of MI Motivational Interviewing Change Talk BehaviorChange
Identifying Change Talk • Desire to change • Ability to change • Reasons for change • Need for change • COMMITMENT to making a change
R: Roll with Resistance • Reluctance and ambivalence are to be acknowledged (and even respected) and not confronted directly • Questions and problems may be turned back to the client for solution • Explicit permission is given to disregard what the interviewer is saying • Resistance supplies energy which can be used therapeutically
E: Express Empathy • Therapist empathy repeatedly shown to be predictor of client success in changing addictive behavior • The operational definition of empathy is reflective listening • Empathy indicates that the speaker has been understood
D: Develop Discrepancy • The discrepancy between client values and current behavior is the location of fruitful therapeutic work • Weighing pros and cons in nonjudgmental fashion will facilitate this discrepancy • The client, not the therapist, must verbalize arguments for change
S: Support Self-efficacy • Efficacy is the belief that a person can make a specific change • Robust predictor of outcomes with a variety of clinical problems • Interviewers may search for optimism in client’s previous successes
Decisional Balance What are the pros of the adolescent’s drug use? ____________________________________________________________________ ____________________________________________________________________ ____________________________________________________________________ ____________________________________________________________________ What are the cons (negatives) of the adolescent’s drug use? ____________________________________________________________________ ____________________________________________________________________ ____________________________________________________________________ What is accomplished with this procedure? ____________________________________________________________________ How does it enhance self-motivation? ____________________________________________________________________ How does it help with establishing goals? ____________________________________________________________________
Outline of Talk • Brief Interventions (BI) • Screening • Motivational Interviewing (MI) • Teen Intervene Update • Case Example
teen-intervene www.hazelden.org
Teen Intervene Update • Latest research data • Implementation • Use in groups • Learning TI • Collecting follow-up data • New parent project (Home Base)
Teen Intervene Update • Latest research data • New summary in NREPP (www.nrepp.samhsa.gov) • Ratings were in the 3-4 range
Teen Intervene Update • Latest research data • New summary in NREPP (www.nrepp.samhsa.gov) • Ratings were in the 3-4 range • Recent publications in scientific literature • SUD sample - 6 and 12 month outcome JSAT and PAB • Truant sample – 18 month outcome JCASA
Teen Intervene Update • SUD sample - 6 and 12-month outcome • Full 3-session version is better than the 2-session (youth only) • although at 12-months, minimal difference • 2-session better than assessment only
Research Abstinence rates at 6-months post-intervention for each of the 3 groups Source: Winters (CPDD, 2008). Notes. Groups: BI-Y = BI-Youth only; BI-YP = BI-Youth and Parent; CON = Control, assessment only.