Download
1 / 1
10 likes | 184 Views
J. P. Gamarnik 1 | K. D. Dwyer 2 | J. Roth 3 | M. Lamontagne 2, 4 jgama061@uottawa.ca | mlamon@uottawa.ca. INTRODUCTION.

E N D
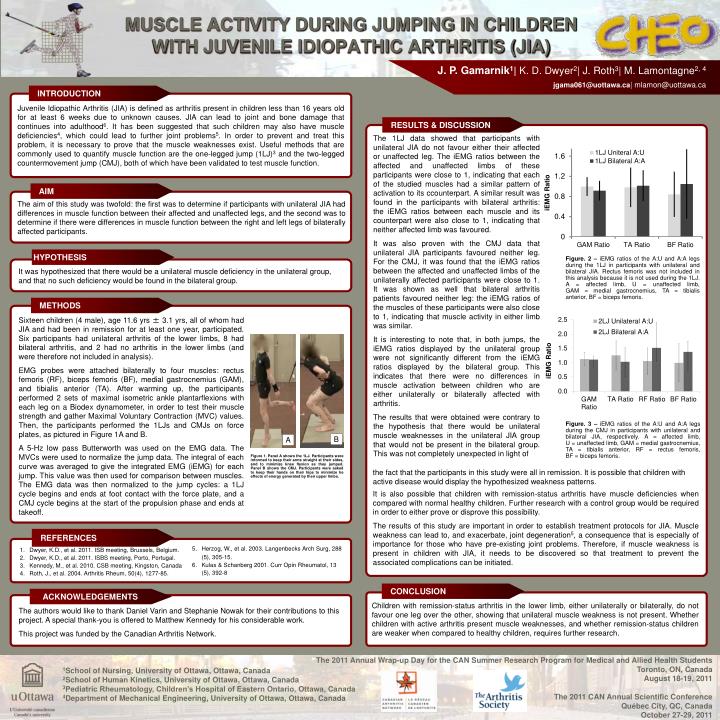
J. P. Gamarnik1| K. D. Dwyer2| J. Roth3| M. Lamontagne2, 4jgama061@uottawa.ca| mlamon@uottawa.ca INTRODUCTION Juvenile Idiopathic Arthritis (JIA) is defined as arthritis present in children less than 16 years old for at least 6 weeks due to unknown causes. JIA can lead to joint and bone damage that continues into adulthood6. It has been suggested that such children may also have muscle deficiencies4, which could lead to further joint problems5. In order to prevent and treat this problem, it is necessary to prove that the muscle weaknesses exist. Useful methods that are commonly used to quantify muscle function are the one-legged jump (1LJ)3 and the two-legged countermovement jump (CMJ), both of which have been validated to test muscle function. RESULTS & DISCUSSION The 1LJ data showed that participants with unilateral JIA do not favour either their affected or unaffected leg. The iEMG ratios between the affected and unaffected limbs of these participants were close to 1, indicating that each of the studied muscles had a similar pattern of activation to its ccounterpart. A similar result was found in the participants with bilateral arthritis: the iEMG ratios between each muscle and its counterpart were also close to 1, indicating that neither affected limb was favoured. It was also proven with the CMJ data that unilateral JIA participants favoured neither leg. For the CMJ, it was found that the iEMG ratios between the affected and unaffected limbs of the unilaterally affected participants were close to 1. It was shown as well that bilateral arthritis patients favoured neither leg: the iEMG ratios of the muscles of these participants were also close to 1, indicating that muscle activity in either limb was similar. It is interesting to note that, in both jumps, the iEMG ratios displayed by the unilateral group were not significantly different from the iEMG ratios displayed by the bilateral group. This indicates that there were no differences in muscle activation between children who are either unilaterally or bilaterally affected with arthritis. The results that were obtained were contrary to the hypothesis that there would be unilateral muscle weaknesses in the unilateral JIA group that would not be present in the bilateral group. This was not completely unexpected in light of AIM The aim of this study was twofold: the first was to determine if participants with unilateral JIA had differences in muscle function between their affected and unaffected legs, and the second was to determine if there were differences in muscle function between the right and left legs of bilaterally affected participants. MUSCLE ACTIVITY DURING JUMPING IN CHILDREN WITH JUVENILE IDIOPATHIC ARTHRITIS (JIA) HYPOTHESIS Figure. 2 – iEMG ratios of the A:U and A:A legs during the 1LJ in participants with unilateral and bilateral JIA. Rectus femoris was not included in this analysis because it is not used during the 1LJ. A = affected limb, U = unaffected limb, GAM = medial gastrocnemius, TA = tibialis anterior, BF = biceps femoris. It was hypothesized that there would be a unilateral muscle deficiency in the unilateral group, and that no such deficiency would be found in the bilateral group. METHODS Sixteen children (4 male), age 11.6 yrs ± 3.1 yrs, all of whom had JIA and had been in remission for at least one year, participated. Six participants had unilateral arthritis of the lower limbs, 8 had bilateral arthritis, and 2 had no arthritis in the lower limbs (and were therefore not included in analysis). EMG probes were attached bilaterally to four muscles: rectus femoris (RF), biceps femoris (BF), medial gastrocnemius (GAM), and tibialis anterior (TA). After warming up, the participants performed 2 sets of maximal isometric ankle plantarflexions with each leg on a Biodex dynamometer, in order to test their muscle strength and gather Maximal Voluntary Contraction (MVC) values. Then, the participants performed the 1LJs and CMJs on force plates, as pictured in Figure 1A and B. A 5-Hz low pass Butterworth was used on the EMG data. The MVCs were used to normalize the jump data. The integral of each curve was averaged to give the integrated EMG (iEMG) for each jump. This value was then used for comparison between muscles. The EMG data was then normalized to the jump cycles: a 1LJ cycle begins and ends at foot contact with the force plate, and a CMJ cycle begins at the start of the propulsion phase and ends at takeoff. Figure. 3 – iEMG ratios of the A:U and A:A legs during the CMJ in participants with unilateral and bilateral JIA, respectively. A = affected limb, U = unaffected limb, GAM = medial gastrocnemius, TA = tibialis anterior, RF = rectus femoris, BF = biceps femoris. B A Figure 1. Panel A shows the 1LJ. Participants were informed to keep their arms straight at their sides, and to minimize knee flexion as they jumped. Panel B shows the CMJ. Participants were asked to keep their hands on their hips to minimize he effects of energy generated by their upper limbs. the fact that the participants in this study were all in remission. It is possible that children with active disease would display the hypothesized weakness patterns. It is also possible that children with remission-status arthritis have muscle deficiencies when compared with normal healthy children. Further research with a control group would be required in order to either prove or disprove this possibility. The results of this study are important in order to establish treatment protocols for JIA. Muscle weakness can lead to, and exacerbate, joint degeneration5, a consequence that is especially of importance for those who have pre-existing joint problems. Therefore, if muscle weakness is present in children with JIA, it needs to be discovered so that treatment to prevent the associated complications can be initiated. REFERENCES 5. Herzog, W., et al. 2003. Langenbecks Arch Surg, 288(5), 305-15. 6. Kulas & Schanberg 2001. Curr Opin Rheumatol, 13 (5), 392-8 • Dwyer, K.D., et al. 2011. ISB meeting, Brussels, Belgium. • Dwyer, K.D., et al. 2011. ISBS meeting, Porto, Portugal. • Kennedy, M., et al. 2010. CSB meeting, Kingston, Canada • Roth, J., et al. 2004. Arthritis Rheum, 50(4), 1277-85. CONCLUSION ACKNOWLEDGEMENTS Children with remission-status arthritis in the lower limb, either unilaterally or bilaterally, do not favour one leg over the other, showing that unilateral muscle weakness is not present. Whether children with active arthritis present muscle weaknesses, and whether remission-status children are weaker when compared to healthy children, requires further research. The authors would like to thank Daniel Varin and Stephanie Nowak for their contributions to this project. A special thank-you is offered to Matthew Kennedy for his considerable work. This project was funded by the Canadian Arthritis Network. The 2011 Annual Wrap-up Day for the CAN Summer Research Program for Medical and Allied Health Students Toronto, ON, Canada August 18-19, 2011The 2011 CAN Annual Scientific Conference Québec City, QC, Canada October 27-29, 2011 1School of Nursing, University of Ottawa, Ottawa, Canada 2School of Human Kinetics, University of Ottawa, Ottawa, Canada 3Pediatric Rheumatology, Children’s Hospital of Eastern Ontario, Ottawa, Canada 4Department of Mechanical Engineering, University of Ottawa, Ottawa, Canada