Download
1 / 35
350 likes | 534 Views
Provider Tips and Toolsets Rural Quality Program Conference Office of Rural Health Policy Health Resources Services Administration September 2, 2009. Kathy Reims, MD Chief Medical Officer CSI Solutions, LLC Clinical Assistant Professor, UCHSC. Eugene Maynard, MD

E N D
Provider Tips and ToolsetsRural Quality Program Conference Office of Rural Health Policy Health Resources Services AdministrationSeptember 2, 2009 Kathy Reims, MD Chief Medical Officer CSI Solutions, LLC Clinical Assistant Professor, UCHSC Eugene Maynard, MD Rural Quality Project Participant Benson Area Medical Center Benson, NC I do not have any relevant financial relationships to disclose
Objectives • Provide practical tools and tips to improve performance on OHRP CVD measures • General approach • Hypertension and Lipid control • Integrated Smoking Cessation Toolkit
Tools to Improve Performance • Patient Factors • Care Team Factors • System Factors
Patient Factors • Awareness* • Education* • Commitment to Care Plan • Patient confidence in managing condition* • Side effects • Practical considerations • Psychosocial impacts*
Assist Patients with Care Plans • Self-Management supports* • Proactive follow up* • Care Team is accessible • DAP programs • Pay attention to medication regimens • Medication reconciliation • Screen for literacy*, depression*, substance abuse
Care Team Factors • Evidence-based care* • Planned Care • POS prompts and reminders* • Protocols • Trained Staff* • Delegated work* • Outreach and proactive follow up* • Expand the team: pharmacist, promotora • Optimize the team: designated roles or FTE*
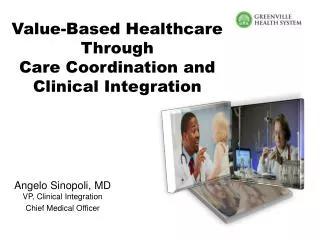
System Factors • Access • Group visits* • Email or Web-based • Convenient, timely appointments • Continuity of care • Population management* • Coordination of care • Effective use of technology*
Awareness: BP Control Rates Trends in awareness, treatment, and control of high blood pressure in adults ages 18–74 Sources: Unpublished data for 1999–2000 computed by M. Wolz, National Heart, Lung, and Blood Institute; JNC 6.
Patient Education http://www.nhlbi.nih.gov/health/public/heart/hbp/dash/dash_brief.pdf
Education and Patient Reminders:National Cholesterol Education Program http://www.nhlbi.nih.gov/health/public/heart/chol/wyntk.pdf
HTN & Lipid Patient Education • http://www.nhlbi.nih.gov/health/index.htm • http://www.americanheart.org/presenter.jhtml?identifier=1516 • http://familydoctor.org/online/famdocen/home/common/heartdisease/risk/092.html • http://www.webmd.com/heart-disease/guide/heart-disease-prevent
Patient Self Management http://www.ama-assn.org/ama1/pub/upload/mm/433/phys_resource_guide.pdf
BUBBLE DIAGRAM If you have diabetes, here are some things many individuals try to do for their health. Would you like to set any goals concerning any of them? Blood glucose monitoring Taking medications to help control blood sugar Skin care Taking insulin Diet Depression Losing weight Daily foot care Smoking
Goal Setting Tools www.healthdisparities.net
Plan the Visit: Flowsheet • Organize key information • POS Reminders • Share the work • Huddles
Evidenced-based Care • ATP III Palm Interactive Guideline Tool http://hp2010.nhlbihin.net/atpiii/atp3palm.htm • CVD Risk Calculator http://hp2010.nhlbihin.net/atpiii/calculator.asp • ATP III At-a-Glance Desk Reference http://www.nhlbi.nih.gov/guidelines/cholesterol/dskref.htm
Staff Training: Lunch and Learns • JNC VII Slide Set http://hp2010.nhlbihin.net/nhbpep_slds/menu.htm • AAFP Ask and Act Program http://www.aafp.org/online/en/home/clinical/publichealth/tobacco/toolkit.html • ATP III Slide Set http://hp2010.nhlbihin.net/ncep_slds/menu.htm
Staff Training: Unified Health Communication 101: Addressing Health Literacy, Cultural Competency, and Limited English Proficiency • Improve your patient communication skills • Increase your awareness and knowledge of the three main factors that affect your communication with patients • Implement patient-centered communication practices
Optimize your Team: Case Manager Role • Plans and integrates care for people with diabetes and other chronic diseases • Liaison with other community resources • Provide good documentation in patient record, all patient contact attempts, and all telephone and written communication with patients • Log in binder the appointment date/time/location; check off if the letter was sent, phone call made, films requested • Reviews charts for what is needed (with help of other team members) • Coordinate with other team members • Help with referrals and links to community resources as needed • Helps counsel around self-management goals
Health Literacy Screen Newest Vital Sign http://www.pfizerhealthliteracy.com/pdf/FH_vitalsigns_040605.pdf
Depression Screening • http://www.commonwealthfund.org/usr_doc/PHQ2.pdf PHQ -9 http://www.depression-primarycare.org/clinicians/toolkits/materials/forms/phq9/
Why Process Map? • Creates a visual snapshot of the current flow of the process • Allows you to “see” opportunities for improvement • Facilitates identification of process variations, duplications and waste • Adds a discipline to improvement • Allows involvement of all key players
Patient given order for fasting lipids Results notification mailed Yes Lipids at target? No Lab gives results to PCP PCP orders follow up visit RN enters patient name and date into log (in lab) But what about….? Returned results are processed by lab staff and results entered into log RN schedules appointment
Patient given order for fasting lipids Results notification mailed Yes Lipids at target? No RN enters patient name and date into log (in lab) • Gaps addressed: • Follow up for Lipid results that have not been returned • Ability to track if patient received timely follow up on elevated lipids. Lab gives results to PCP. PCP orders follow up visit. Log checked q 2 weeks for follow up phone calls needed RN schedules appointment and places reminder in tickler file Returned results are processed by lab staff and results entered into log Front desk checks tickler and reports no-show appointment to RN
Smoking Cessation Toolkit An Integrated Approach