Download
1 / 29
290 likes | 366 Views
Changes in ASD Rates In Utah from 2002-2010: Explanations for increases?. Judith Pinborough Zimmerman, Ph.D. Assistant Research Professor University of Utah judith.zimmerman@hsc.utah.edu. Background.

E N D
Changes in ASD Rates In Utah from 2002-2010: Explanations for increases? Judith Pinborough Zimmerman, Ph.D. Assistant Research Professor University of Utah judith.zimmerman@hsc.utah.edu
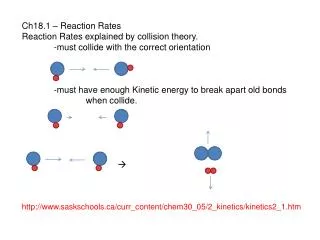
Background • Autism spectrum disorders (ASDs) are a group of developmental disabilities characterized by impairments in social interaction and communication, as well as restricted, repetitive, and stereotyped patterns of behavior • Cause is unknown • Genetics and environmental susceptibility • Challenges in determining the prevalence of autism • More affected versus more detected?
ASD Prevalence: Who, where, and how you count counts • Retrospective record reviews (Centers for Disease Control and Prevention Autism and Developmental Disabilities Monitoring Network) • 1 in 47 in 2008 study year • Administrative counts • Surveys • Direct Screening and Assessment
Variation across Sites in Identified Prevalence of ASDsADDM Network, 14 Sites, 2008 (MMWR, 2012) Identified ASD Prevalence per 1,000 Health-Only Records Access Education & Health Records Access
Change in Identified Utah ASD Prevalence by Intellectual Ability
Associated Features Eating Sleeping Mood Discrepancy in cognitive profile Aggression Oppositional Motor delays Hyperactivity Lack or excessive fear Odd responses to sensory stimuli Self injurious behavior Seizures/staring spells Temper tantrums
Earliest Known Utah ASD DiagnosisMedian Age and Proportion by Diagnostic Subtype Limitations: Diagnostic information obtained from evaluation records may not capture the exact age of each child’s earliest diagnosis Instability of diagnostic subtypes over time
Utah ASD Administrative Prevalence * 2002-2008 includes Davis, Salt Lake, and Utah counties. † 2010 includes Davis, Salt Lake, Tooele, and Utah counties. Source: Pinborough-Zimmerman, J., Intveld, A., Kingsbury, C.M.B. Changes in the Administrative Prevalence of Autism Spectrum Disorders in Utah from 2002-2010, University of Utah, 2012.
ASD Prevalence: Use of surveys • Survey: caregiver report of ASD diagnosis. • 2011 National Survey of Children’s Health telephone survey found 2% of 6 to 17 year olds had a diagnosis of ASD compared to the 2007 estimate of 1.16 % • Increase was greater for boys than girls, and among 14-17 years olds than younger children • Attribute change to doctors better identifying the disorder
ASD Prevalence: Direct Assessment • Direct Assessment: Screening & comprehensive assessment of a population by clinicians. The “gold standard”. • Kim et al., (Am J Psychiatry, 2011) screened and evaluated 7-12 year olds in a town in South Korea (n=55,000). Reported a prevalence of 1 in 38 or 2.64% • Brugha et al., (Arch Gen Psychiatry, 2011 ) conducted diagnostic assessments in an adult population in England (n=7461) and found 1% prevalence without a significant reduction in the older part of the sample
Factors that may influence ASD prevalence trends • Intrinsic Identification: internal methodology or measurement factors • Extrinsic Identification: external classification and awareness factors involved in identifying people with ASD in a population • Risk: Possible etiologic or true change in ASD symptoms among the population
Chemical Pollutants and Autism • Traffic related air pollution • Volk et al (JAMA, 2013) Exposure to traffic related air pollution, nitrogen dioxide, PM2.5 and PM 10 during pregnancy was associated with autism (AOR, 1.98 during gestation and 3.10 during first year of life) • Becerra et al., (Environ Health Perspect, 2013) Association between autism and prenatal air pollution exposure related to traffic sources • Windham et al ((Environ Health Perspect, 2013) potential association between autism and estimated metal concentrations and possibly solvents in ambient air around birth residence
Maternal Residential Proximity to Toxic Release Inventory Sites • Identified by 2002 UT-ADDM (CDC, 2007; Pinborough-Zimmerman, et al, 2009; Pinborough-Zimmerman, et al., 2007) • Children living in Salt Lake, Davis, or Utah Counties in 2002 (born in 1994) • Cases were matched to Utah birth records using a deterministic and probabilistic hybrid approach • 99% of maternal birth addresses geocoded for cases and controls
Sites listed in a publicly available EPA database • contains information on toxic chemical releases and waste management activities reported annually • TRI sites operational in 1993-1994 with annual reportable emissions of heavy metals (arsenic, cadmium, lead, nickel, and mercury) and halogenated chemicals (dioxins, PCB’s, trichloroethylene) • Geocoded sites (n=54) (EPHT) Toxic Release Inventory Sites
Type of Exposure Contaminant Level 1 = Heavy Metals 1 = < 250 lbs 2 = Halogenated Chemicals 2 = > 250 < 5,000 lbs 3 = Both 3 = > 5,000 < 10,000 lbs 4 = > 10,000 lbs Chemical Type and Poundage
Primary Aim: • Created buffer zones (¼, ½ and 1 mile) around TRI facilities • Compared the proportion of cases vs. controls by buffer distance, case type, chemical group, and poundage level • Tested for significant difference Analysis
Completeness of case ascertainment Population-based sample Geocoded maternal addresses for cases and controls Site specific addresses of TRI sites, chemical and poundage type Multiple measures of SES Strengths
Addresses for the first trimester of pregnancy are unknown Exposure estimates do not include other sources of chemical exposures Chemical concentrations represent annual measures by site No actual personal measurements in subjects Unable to take into account mobility or specific maternal activities Findings are preliminary and further analysis needed Limitations
Service and Research Implications • Better identification among certain subgroups • Still concerned about disparities in identified prevalence • Across sites (methodological: access to records / geographic: access to care) • Among children of minority race/ethnicity, low socioeconomic status • More children than ever are being recognized as having ASDs • Still concerned that 20% are not classified with autism by community providers, others are not recognized as early as they can be • Need to accelerate our research into risk factors and causes of ASD • Highlights the need for further scientific investigation into the potential association of exposure to hazardous air pollutants and increased risk of ASD and other developmental disabilities