Download
1 / 1
10 likes | 69 Views
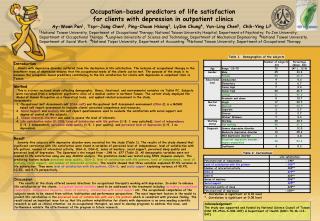
Childhood food allergies are an increasingly common health concern that affects approximately 6% to 8% of children in the United States (Gupta et al., 2009). Reaction to food allergens can range from mild to severe and may even result in death due to anaphylaxis (Branum & Lucaks, 2008).

E N D
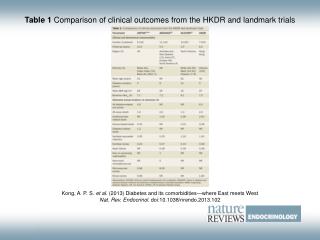
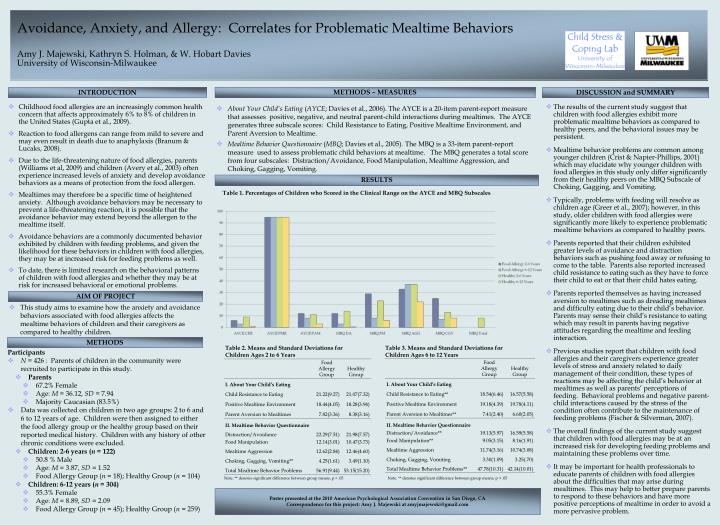
Childhood food allergies are an increasingly common health concern that affects approximately 6% to 8% of children in the United States (Gupta et al., 2009). Reaction to food allergens can range from mild to severe and may even result in death due to anaphylaxis (Branum & Lucaks, 2008). Due to the life-threatening nature of food allergies, parents (Williams et al, 2009) and children (Avery et al., 2003) often experience increased levels of anxiety and develop avoidance behaviors as a means of protection from the food allergen. Mealtimes may therefore be a specific time of heightened anxiety. Although avoidance behaviors may be necessary to prevent a life-threatening reaction, it is possible that the avoidance behavior may extend beyond the allergen to the mealtime itself. Avoidance behaviors are a commonly documented behavior exhibited by children with feeding problems, and given the likelihood for these behaviors in children with food allergies, they may be at increased risk for feeding problems as well. To date, there is limited research on the behavioral patterns of children with food allergies and whether they may be at risk for increased behavioral or emotional problems. The results of the current study suggest that children with food allergies exhibit more problematic mealtime behaviors as compared to healthy peers, and the behavioral issues may be persistent. Mealtime behavior problems are common among younger children (Crist & Napier-Phillips, 2001) which may elucidate why younger children with food allergies in this study only differ significantly from their healthy peers on the MBQ Subscale of Choking, Gagging, and Vomiting. Typically, problems with feeding will resolve as children age (Greer et al., 2007); however, in this study, older children with food allergies were significantly more likely to experience problematic mealtime behaviors as compared to healthy peers. Parents reported that their children exhibited greater levels of avoidance and distraction behaviors such as pushing food away or refusing to come to the table. Parents also reported increased child resistance to eating such as they have to force their child to eat or that their child hates eating. Parents reported themselves as having increased aversion to mealtimes such as dreading mealtimes and difficulty eating due to their child’s behavior. Parents may sense their child’s resistance to eating which may result in parents having negative attitudes regarding the mealtime and feeding interaction. Previous studies report that children with food allergies and their caregivers experience greater levels of stress and anxiety related to daily management of their condition, these types of reactions may be affecting the child’s behavior at mealtimes as well as parents’ perceptions of feeding. Behavioral problems and negative parent-child interactions caused by the stress of the condition often contribute to the maintenance of feeding problems (Fischer & Silverman, 2007). The overall findings of the current study suggest that children with food allergies may be at an increased risk for developing feeding problems and maintaining these problems over time. It may be important for health professionals to educate parents of children with food allergies about the difficulties that may arise during mealtimes. This may help to better prepare parents to respond to these behaviors and have more positive perceptions of mealtime in order to avoid a more pervasive problem. Avoidance, Anxiety, and Allergy: Correlates for Problematic Mealtime BehaviorsAmy J. Majewski, Kathryn S. Holman, & W. Hobart DaviesUniversity of Wisconsin-Milwaukee METHODS – MEASURES INTRODUCTION DISCUSSION and SUMMARY • About Your Child’s Eating (AYCE; Davies et al., 2006). The AYCE is a 20-item parent-report measure that assesses positive, negative, and neutral parent-child interactions during mealtimes. The AYCE generates three subscale scores: Child Resistance to Eating, Positive Mealtime Environment, and Parent Aversion to Mealtime. • Mealtime Behavior Questionnaire (MBQ; Davies et al., 2005). The MBQ is a 33-item parent-report measure used to assess problematic child behaviors at mealtime. The MBQ generates a total score from four subscales: Distraction/Avoidance, Food Manipulation, Mealtime Aggression, and Choking, Gagging, Vomiting. RESULTS Table 1. Percentages of Children who Scored in the Clinical Range on the AYCE and MBQ Subscales AIM OF PROJECT • This study aims to examine how the anxiety and avoidance behaviors associated with food allergies affects the mealtime behaviors of children and their caregivers as compared to healthy children. METHODS Table 2. Means and Standard Deviations for Children Ages 2 to 6 Years Table 3. Means and Standard Deviations for Children Ages 6 to 12 Years • Participants • N = 426 : Parents of children in the community were recruited to participate in this study. • Parents • 67.2% Female • Age: M = 36.12, SD = 7.94 • Majority Caucasian (83.5%) • Data was collected on children in two age groups: 2 to 6 and 6 to 12 years of age. Children were then assigned to either the food allergy group or the healthy group based on their reported medical history. Children with any history of other chronic conditions were excluded. • Children: 2-6 years (n = 122) • 50.8 % Male • Age: M = 3.87, SD = 1.52 • Food Allergy Group (n = 18); Healthy Group (n = 104) • Children: 6-12 years (n = 304) • 55.3% Female • Age: M = 8.89, SD = 2.09 • Food Allergy Group (n = 45); Healthy Group (n = 259) Note. ** denotes significant difference between group means, p < .05 Note. ** denotes significant difference between group means, p < .05 Poster presented at the 2010 American Psychological Association Convention in San Diego, CACorrespondence for this project: Amy J. Majewski at amyjmajewski@gmail.com