Download
1 / 21
210 likes | 635 Views
GUIDELINES & TOOLS for HOSPITAL DOTS LINKAGE (HDL). TBCAP project C3 APA2 PPM Sub-group meeting, Cairo Jan Voskens. Challenges to DOTS in hospitals. Inadequate clinical management practices no standardized protocols for diagnosis and treatment of TB

E N D
GUIDELINES & TOOLS for HOSPITAL DOTS LINKAGE(HDL) TBCAP project C3 APA2 PPM Sub-group meeting, Cairo Jan Voskens
Challenges to DOTS in hospitals • Inadequate clinical management practices • no standardized protocols for diagnosis and treatment of TB • poor case holding and high rates of default • lack of resources and linkages • user fees • multiple services: TB suspects and TB patients identified in different units Risk for amplification of MDR !!
Definition Hospital DOTS Linkage HDL building a network between public and private clinical care facilities, (including primary, secondary and tertiary hospitals, academic hospitals and charity/ NGO hospitals ) and the national DOTS program
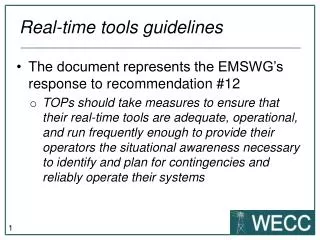
Overall objectives • Ensure access to quality DOTS services for TB patients seeking care within the hospital sector based on International Standards of Tuberculosis Care (ISTC). • Enable hospitals (public and private, governmental and non-governmental) to implement TB control activities that are linked to the NTP
Specific objectives • ISTC endorsed and implemented by public and private hospital providers • Decreased diagnostic delays and cost savings to patients • Effective referral mechanism established • Improved monitoring of treatment and treatment outcomes for patients diagnosed in hospitals • Improved hospital laboratory quality assurance • Enhanced surveillance to measure performance
GovernmentNTP Partners Local Stop TB Partnership Health Office Providers: Private, NGO’s,etc Professional Organisations COORDINATING BODY: HDL team Districts Hospitals pp pp pp pp pp Health Centers HDL Framework
Steps for HDL • Planning • Implement the external network • Implement the internal network • Monitoring and evaluation
I. role of the central level • determine overall policy direction (i.e. national guidelines and standards) • formulate regulatory frameworks (certification) Steps: • establish coordination of stakeholders: public-, private, NGO, medical schools, professional societies etc • build commitment among decision makers • develop implementation plan including • human resource development • enablers • monitoring and evaluation • mobilize resources • monitor and evaluate
enablers • Free anti-TB medications • Training and in-service updates for staffs • Commodities supplied: surveillance, IEC materials, diagnostic supplies and equipment • Logistical support for laboratory EQA network • Corporate social responsibility to participate in NTP • Certification and accreditation
II. Steps to build HDLexternal Network • Advocate and mobilize resources • Establish local coordinating body for HDL • Define Terms of Reference for interagency collaborations (MoU) • Carry out baseline assessment of facilities • Develop implementation plan including • HRD • Establishing referral system • Supervision and problem solving support
Referral system for patients diagnosed in hospitals • Develop SOP for patient referral • Appoint ‘’referral coordinator’’ • implement tools: • Patient referral– and Referral feedback forms – • Patient referral register/log kept by referral coordinator • Default tracing form and Default tracing register/log • Telephone directory of surrounding health facilities
Generic referral mechanism Notification of referral Feed back of information Referral register Referral Coordinator Phone directory SMS, phone Receiving Health facility ‘B’ Referring hospital ‘A’
Indicators: • Confirmed sputum diagnosis rate: No. pts. diagnosed in hospital with smear confirmation X 100 % No. of patients diagnosed by hospital • Successful referral rate: No. of patients received at DOTS center X 100 % No. of patients referred by hospitals • Successful referral tracing rate: No. of patients retrieved for treatment X 100 % No. of patients that dropped out after referral Other useful indicators: • Treatment outcomes of referred patients (compared to not referred pts) • Referral coordinator appointed and in place • Percentage of hospitals implementing SOP for patient referral • Availability of telephone directory of facilities in cluster area (province, district)
III. Steps to build HDL Internal Network (a) • Baseline assessment and planning of Internal Network • Assess existing hospital practicesand give feedback • Development of a specified HDL task mix • hospital implementation plan • Sensitization and advocacy • Create hospital task force or DOTS committee • hospital directive and/or district or local NTP-hospital MOU • Establish Hospital DOTS Unit (DOTS executive room)
GENERAL CLINICS and WARDS SPECIALIZED LABORATORY CLINICS and PATIENT RADIOLOGY WARDS incl VCT/ART EMERGENCY PATHOLOGY ROOM Ho spital DOTS UNIT & DOTS team PHARMACY MEDICAL RECORD HOSPITAL IEC Community OTHER (i.e. SOCIAL Others Health SERVICES) Centre Internal network
Steps to build HDL Internal Network (b) • Define SOP for • TB case management (diagnosis / treatment) • Patient referral • Internal (within facility) • External (to local TB treatment centers) • Develop HRD plan (based on selected task mix and SOP) • Integrate hospital laboratory into the EQA network of the NTP • Ensure proper surveillance and supervision
Public health functions of options 3 and 4 are variable and are normally context –specific
Scaling up • Phased wise expansion • Supervision: monitor hospital performance continuously to assure QUALITY !!!
Thank you! Your comments and inputs on this draft are most welcome