Download
1 / 33
410 likes | 847 Views
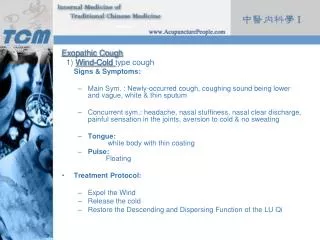
COUGH AND COLD PREPARATIONS. ANTIHISTAMINE Diphenhydramine DECONGESTANTS MUCOLYTICS Acetylcysteine EXPECTORANTS Guaifenesin COUGH SUPPRESSANTS Codeine DM ( dextromethorphan ).

E N D
COUGH AND COLD PREPARATIONS • ANTIHISTAMINE Diphenhydramine • DECONGESTANTS • MUCOLYTICS Acetylcysteine • EXPECTORANTS Guaifenesin • COUGH SUPPRESSANTS Codeine DM (dextromethorphan)
Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease NHLBI/WHO Global Initiative for Chronic Obstructive Lung Disease (GOLD) Workshop Summary 2008 • Mucolytic (mucokinetic, mucoregulator) agents. (ambroxol, erdosteine, carbocysteine, iodinated glycerol): Although a few patients with viscous sputum may benefit from mucolytics (124, 125), the overall benefits seem to be very small. Therefore, the widespread use of these agents cannot be recommended on the basis of the present evidence (Evidence D).
There is no evidence to support the use of heliox, DNase or mucolytics for the treatment of acute asthma in childhood. • UK, Feb 2009 British Guideline on the Management of Asthma, 2008
Antihistamines Drugs that directly compete with histamine for specific receptor sites • Two histamine receptors • H1 (histamine1) • H2 (histamine2) • H1 histamine receptor- found on smooth muscle, endothelium, and central nervous system tissue; causes vasodilation, bronchoconstriction, smooth muscle activation, and separation of endothelia cellss (responsible for hives), and pain and itching due to insect stings H1 antagonists are commonly referred to as antihistamines • Antihistamines have several properties • Antihistaminic • Anticholinergic • Sedative
Antihistamines: Indications Management of: • Nasal allergies • Seasonal or perennial allergic rhinitis (hay fever) • Allergic reactions • Motion sickness • Histamine-mediated disorders • Allergic rhinitis (hay fever, mould and dust allergies) • Anaphylaxis • Angioneurotic edema • Drug fevers • Insect bite reactions • Urticaria (itching)
ACCP Cough guideline • Patients with acute cough (as well as postnasal drip [PND] and throat clearing) associated with the common cold can be treated with a first-generation antihistamine/decongestant (A/D) preparation (brompheniramine and sustained-release pseudoephedrine). Naproxen can also be administered to help decrease cough in this setting. Level of evidence, fair; benefit, substantial; grade of recommendation, A • In patients with the common cold, newer generation nonsedating antihistamines are ineffective for reducing cough and should not be used. Level of evidence, fair; benefit, none; grade of recommendation, D Pratter MR. Cough and the common cold: ACCP evidence-based clinical practice guidelines. Chest 2006 Jan;129(1 Suppl):72S-4S.
Antihistamines Ex: Diphenhydramine, chlorphenamine, brompheniramine MOA: H1 blocker; competes with receptor sites in resp. tract, GI, blood vessels Adv eff: • CNS drowsiness, headache, fatigue, nervousness, dizziness • Anticholinergic (drying) effects, most common • Dry mouth • Difficulty urinating • Constipation • Changes in vision • Arrhythmia, hallucinations, heart block, paradoxic excitability, respiratory depression, sedation, tachycardia, • GIT: appetite increase, weight gain, diarrhea, n/v • Arthralgia, pharyngitis
Antihistamines: • Contraindicated in the presence of acute asthma attacks and lower respiratory diseases • Use with caution in increased intraocular pressure, cardiac or renal disease, hypertension, asthma, COPD, peptic ulcer disease, BPH, or pregnancy
Nonsedating/Peripherally Acting Antihistamines • Developed to eliminate unwanted side effects, mainly sedation • Work peripherally to block the actions of histamine; thus, fewer CNS side effects • Longer duration of action (increases compliance) • Examples: cetirizine (virlix), fexofenadine(allegra)
ACCP Evidence-based Clinical Practice Guidelines, • In patients with the common cold, newer generation nonsedating antihistamines are ineffective for reducing cough and should not be used. Level of evidence, fair; benefit, none; grade of recommendation, D Pratter MR. Cough and the common cold: ACCP evidence-based clinical practice guidelines. Chest 2006 Jan;129(1 Suppl):72S-4S.
Oral Decongestants • Prolonged decongestant effects, but delayed onset • Effect less potent than topical • No rebound congestion • MOA: Exclusively adrenergics • Example: pseudoephedrine, Sinutab, Dristan, Tylenol cold, Sudafed • Adverse effect: agitation, anorexia, dysrhythmia, dystonic reactions, headache, hypertension, irritability, nausea, palpitations, seizure, sleeplessness, tachycardia, vomiting
Phenylpropanolamine has been associated with an increased risk of hemorrhagic stroke (bleeding into the brain or into tissue surrounding the brain) in women. Men may also be at risk. Although the risk of hemorrhagic stroke is low, the U.S. Food and Drug Administration (FDA) recommends restricted use of phenylpropanolamine.
Topical Nasal Decongestants • MOA: Adrenergics • Constrict small blood vessels that supply URI structures • As a result these tissues shrink, and nasal secretions in the swollen mucous membranes are better able to drain • Topical adrenergics • Prompt onset • Potent • Sustained use over several days causes rebound congestion, making the condition worse • COMPOSITION:Each 1 mL of solution contains:PhenylephrineHCl 5 mgPheniramineMaleate 2 mg
Nasal Decongestants: • Decongestants may cause hypertension, palpitations, and CNS stimulation • Repeated use of nasal decongestants causes a decreased sensitivity to their vasoconstrictor effect and a rebound phenomenon with increased nasal congestion and discharge. • Clients on medication therapy for hypertension should check with their physician before taking OTC decongestants • Assess for drug allergies
Topical Nasal Decongestants (cont’d) • Intranasal steroids • beclomethasone dipropionate • flunisolide • fluticasone
Mucolytics ACETYLCYSTEINE MOA: free sulfhydryl grp opens up disulfide bonds in mucoproteins = ↓ viscosity Adv rxns: GI n/v; unpleasant odor CNS: drowsiness, chills Resp: bronchospasm, rhinorrhea, hemoptysis local irritation, clamminess, rash Dose: 1 sachet through inh.
MucolyticAmbroxol • MOA: breakdown of acid mucopolysaccharide fibers; stimulates synthesis and release of surfactant by type II pneumocytes; stimulates the ciliary activity thereby improving mucokinesis (transport of mucous), • Ambroxol is a metabolite of bromhexine • Adv effects: allergic responses such as skin eruption, urticaria or engioneurotic edema may occur. While used for a long time, epigastric pain, nausea and dizziness may occur.
Expectorants: Reflex stimulation • Agent causes irritation of the GI tract • Loosening and thinning of respiratory tract secretions occur in response to this irritation • Example: guaifenesin Direct stimulation • The secretory glands are stimulated directly to increase their production of respiratory tract fluids • Examples: iodine-containing products such as iodinated glycerol and potassium iodide
COUGH AND COLD PREPARATIONSExpectorants GUAIFENESIN MOA: stimulates resp tract secretions = ↑ secretions ↓ viscosity Adv rxns: GI n/v, stomach pains CNS drowsiness, headaches Rashes Dose:100 mg q 4-6
COUGH AND COLD PREPARATIONSANTITUSSIVES: OPIOIDS CODEINE MOA:: central; depression of medullary center binds to opiate receptors in the CNS, = altered perception & response to pain Analgesic / Narcotic / Antitussive Adv effects CNS: drowsiness, dizziness, light- headedness, malaise, headache, restlessness CNS depression Resp: shortness of breath, dyspnea CVS: tachycardia or bradycardia, hypotension GIT: anorexia, nausea, vomiting Hepatic: altered liver enzymes (ALT, AST) gut: decreased iromatopm. Iretera; spasm Derma: rash, urticaria, burning at IV site Dose: 30 mg q 6-8h; SR 60 mg BID max 120 mg/day
COUGH AND COLD DRUGSANTITUSSIVES DEXTROMETHORPHAN (DM) MOA: central: depresses medullarycenter but lacking narcotic properties exc in overdose • Suppress the cough reflex by numbing the stretch receptors in the respiratory tract and preventing the cough reflex from being stimulated Adv reactions CNS: drowsiness, dizziness, coma Resp depression GIT: n/v, constipation, abdominal discomfort Dose: 10-20mg q 4 or 30 mg q 6-8
OTC Restrictions for cough and cold preparations • Medicine and Healthcare products Regulatory Agency in the UK has banned the sale of over the counter cough and cold medicines for babies and young children under the age of 2 as a precautionary measure against accidental overdose because of an increase in reports of adverse reactions linked to overdose. • The cough and cold medicines which will no longer be licensed for children under the age of 2 years, contain the ingredients: • brompheniramine, chlorphenamine & diphenhydramine (antihistamines); • dextromethorphan and pholcodine (antitussives); • guaifenesin and ipecacuanha (expectorants); • phenylephrine, pseudoephedrine, ephedrine, oxymetazoline and xylometazoline (decongestants). Royal Pharm Society Great Brit, Mar 2009
OTC cough and cold restrictions • Health Canada has advised the public that certain over-the-counter cough and cold medicines should not be used in children under 6 years of age, following a review of additional data. The Agency also says that cough and cold medicines marketed for use in children will require enhanced labelling and packaging and that it is working with manufacturers to revise the labelling of these products. • New Zealand(2). In December 2007, the Medicines Adverse Reactions Committee (MARC) reviewed the safety and efficacy of cough and cold medicines in children and recommended that these products should be contraindicated in children under two years of age, based on limited evidence for efficacy in this age group, an absence of evidence-based dosing, and evidence of significant toxicity in overdose. • The affected products are those containing bromhexine, brompheniramine, chlorpheniramine, dextromethorphan, diphenhydramine, doxylamine, guaifenesin, ipecacuanha, oxymetazoline, phenylephrine, pholcodine, promethazine, pseudoephedrine, triprolidine and xylometazoline. No.2, 2009
COUGH AND COLD PREPARATIONS • COMBINATION PREPARATIONS Colvan: DM + Guaifenesin + Chlorpheniramine + paracetamol Dynatussin DM + Guaifenesin + Phenylpropanolamine + Na citrate Tuseran DM + phenylpropanolamine + guiafenesin EurocofGuaiafenesin + chlorpheniramine + Na citrate
ACCP cough guideline • In patients with cough and acute upper respiratory tract infection (URTI), because symptoms, signs, and even sinus imaging abnormalities may be indistinguishable from acute bacterial sinusitis, the diagnosis of bacterial sinusitis should not be made during the first week of symptoms. (Clinical judgment is required to decide whether to institute antibiotic therapy.) Level of evidence, fair; benefit, none; grade of recommendation, D Pratter MR. Cough and the common cold: ACCP evidence-based clinical practice guidelines. Chest 2006 Jan;129(1 Suppl):72S-4S.
Management of Stable COPD Other Pharmacologic Treatments • Antibiotics: Only used to treat infectious exacerbations of COPD • Antioxidant agents: No effect of n-acetylcysteine on frequency of exacerbations, except in patients not treated with inhaled glucocorticosteroids • Mucolytic agents, Antitussives, Vasodilators: Not recommended in stable COPD
The art of medicine consists of amusing the patient while nature cures the disease. - Voltaire