Download

1 / 33
340 likes | 524 Views
Blood Groups and Clotting DN8 Viv Rolfe. Summary. Blood transfusion History of transfusions and what they are used for. ABO blood group system. Rhesus blood group system. Mechanisms of blood clotting. Why give blood?. Why give blood? Because it saves lives. How it is used?.

E N D
Blood Groups and Clotting DN8 Viv Rolfe
Summary • Blood transfusion • History of transfusions and what they are used for. • ABO blood group system. • Rhesus blood group system. • Mechanisms of blood clotting
How it is used? • Whole blood - in extreme emergencies of huge blood loss. • Red cells - anaemia, burn victims, cancer, sickle cell disease. • Platelets - bone marrow failure, leukaemia patients, chemotherapy. • Fresh plasma - blood loss after childbirth, major surgery. • Processed plasma - e.g. factor VIII for treatment of haemophilia.
Blood Typing Blood types must be matched for donation to be successful.
Blood Typing • Many different ways of classifying blood. • Easily tested for using commercially available kits. • ABO/Rhesus both based on the types of ANTIGEN and ANTIBODY in the blood.
Antigen and Antibody ANTIBODY An immunoglobulin protein secreted byour immune system to bind to (and combat) antigen. ANTIGEN A molecule on thesurface of foreign cells (bacteria, viruses) and our own cells (blood, immune) Y Y Y Y Y Y
ABO System • Based on the types of • Antigen markers on red blood cells. • Antibodies in the plasma. What are the 4 types? What type are you?
UK Distribution • A = 42% • B = 8% • AB = 4% • O = 46%
ABO Types of Antigen A antigens B antigens Both Neither
A A Type A blood CAN BE GIVEN to a Type A patient. (B to B, AB to AB and O to O). DONOR RECIPIENT A Anti-B
Type A blood CAN’T BE GIVEN to a Type B patient. • Donated red cells are attacked by recipient’s anti-A antibody in their plasma. B A DONOR RECIPIENT Anti-A
O O B A AB O can be given to EVERYONE (universal donor) O cells have no ANTIGEN
O B A AB AB AB can receive from EVERYONE (universal recipient)
Incompatibility • Reacting cells clump together or AGGLUTINATE. • Can block capillaries stopping the blood flow. • Red blood cells finally rupture - HAEMOLYSIS - releasing HAEMOGLOBIN which is toxic. • Can cause kidney damage and shock (loss of blood to vital organs) and can be fatal.
ABO Interactions Need the same donor or O Universal recipient Universal donor
Summary O A B AB
Rhesus System • First identified in Rhesus monkeys. • Based on the Rhesus antigen on red blood cells. • Rh + people have Rh antigen (85% UK population) • RH - don’t (15% population) BUT CAN DEVELOPANTIBODY IF EXPOSED TO RH+.
So What? • Complications can occur during pregnancy. A Rh- mother with Rh+ baby are at risk…. • Rh- mothers can destroy the baby's blood if this is the 2nd or 3rd pregnancy. • The baby may have to receive a blood transfusion immediately after birth.
http://nobelprize.org/medicine/educational/landsteiner/index.htmlhttp://nobelprize.org/medicine/educational/landsteiner/index.html
Haemostasis • Important to stop haemorrhage. • Must remain localised. • 3 stages: • Vascular spasm • Platelet plug formation • Blood coagulation (clotting)
1 Vascular Spasm • Blood vessels contract. • Reduces blood loss for up to 30 minutes. http://www.mhhe.com/biosci/esp/2002_general/Esp/folder_structure/tr/m1/s7/trm1s7_3.htm
2 Platelet Plug Formation • Plug to prevent blood loss in small vessels.
Platelets release chemicals Serotonin (5-HT) causes vasoconstriction. Thromboxane A2 causes further platelet aggregation.
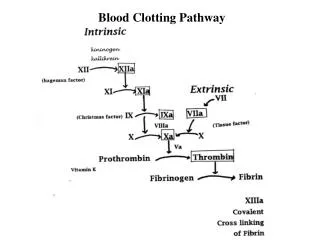
3 Blood Coagulation • Blood thickens forming a gel/clotto prevent loss. • Vitamin K essential for blood clotting. • Chemical reactions for blood clotting are very complex and involve CLOTTING FACTORS.
Extrinsic pathway Intrinsic pathway Occurs in minutes. Chain reaction triggered“within” the blood. FACTOR 11 and 12 Occurs in seconds. Triggered by enzymes “outside” the blood. FACTOR 3 and 7 Thrombin Prothrombin FACTOR 10 Prothrombin activator Fibrin Dense Fibrin Threads FACTOR 13
And afterwards… • Fibrin clot retracts pulling the damagededges together. • The blood clot dissolves.
Problems - Thrombosis • Clot forms in a blood vessel e.g. deep vein thrombosis in legs. • Can cut off oxygen supply causing tissue damage. • Some might dislodge forming an EMBOLUS which can block smaller vessels in the brain or lungs (pulmonary embolism).
Anticoagulants Warfarin - prevents prothrombin formation Heparin - inactivates thrombin Streptokinase - dissolves clots “clot buster”