Download
1 / 39
1.52k likes | 9.54k Views
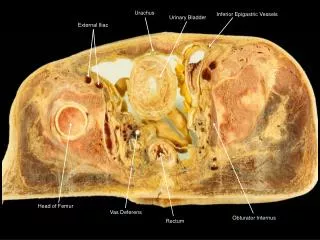
RIGHT ILIAC FOSSA MASS. By, Prof R.A.Pandyaraj , MS, FICS,FAIS,FMAS( Laproscopy ). Head of surgery department, Govt. Royapettah Hospital. BOUNDARIES; TRANS TUBERCULAR LINE MIDCLAVICULAR LINE ILIAC CREST. CONTENTS; Appendix Caecum Mesoappendix Terminal ileum

E N D
RIGHT ILIAC FOSSA MASS By, Prof R.A.Pandyaraj, MS, FICS,FAIS,FMAS(Laproscopy). Head of surgery department, Govt. Royapettah Hospital.
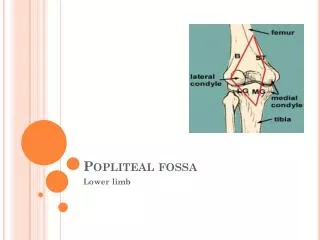
BOUNDARIES; • TRANS TUBERCULAR LINE • MIDCLAVICULAR LINE • ILIAC CREST
CONTENTS; • Appendix • Caecum • Mesoappendix • Terminal ileum • Retro peritoneal tissue • iliac nodes • iliac arteries
APPROACH • INSPECT • PALPATE • PERCUSS • AUSCULTATE • PV / PR • OTHER MASS
PAIN • Dullaching • Colicky • Continuous / intermittent
CLASSIFICATION • ANATOMICAL • Pariteal • Intra abdominal • intra peritoneal • retro peritoneal • CLINICAL • solid mass • cystic mass
ANATOMICAL • INTRA • ABDOMINAL • PARIETAL • LIPOMA • DESMOID TUMOR • PYOGENIC ABSCESS • INTRA ABDOMINAL ABSCESS BURROWING THROUGH • ILIAC ABSCESS • APPENDICULAR ABSCESS
ANATOMICAL • INTRA • ABDOMINAL • PARIETAL APPENDICULAR MASS APPENDICULAR ABSCESS ILEOCAECAL TB CARCINOMA CAECUM MESENTRIC NODES ILIAC NODES TYPHILITIS CROHN’S DISEASE ACTINOMYCOSIS HUGE GALL BLADDER c LIVER INTUSSUSCEPTION AMOEBOMA FEMALES OVARIAN CYST TUBO OVARIAN MASS FIBROID
RETRO PERITONEAL • ANATOMICAL • INTRA • ABDOMINAL • PARIETAL NORMAL SARCOMA ANEURYSM PSOAS ABSCESS TUMOR FROM BONE/ CARTILAGE ABNORMAL UNDESCENDED TESTIS UNASCENDED KIDNEY
CLINICAL • SOLID • CYSTIC • APPENDICULAR ABSCESS • PSOAS ABSCESS • RT.OVARIAN CYST • ILIAC ARTERY ANEURSYM • APPENDICULAR MASS • CARCINOMA CAECUM • ILEO-CAECAL TUBERCULOSIS • EXTERNAL ILLAC LYMPHADENITS • RETRO PERITONEAL SARCOMA • CROHN’S • UNASCENDED KIDNEY • ACTINOMYCOSIS
INVESTIGATIONS • Blood HB , TC,DC,ESR • RFT • X-Ray – Chest,Abdomen Erect • Barium Enema • USG Abdomen • CT Scan Abdomen
APPENDICULAR MASS This is caused by inflammation and swelling of the appendix, caecum, omentum and distal part of the terminal ileum • Treat conservatively with bowel rest, antibiotics, analgesics and fluids • Consider interval appendicectomy if symptoms recur
APPENDICULAR MASS Approach AOSCHNER REGIMEN Initial conservative treatment followed by interval appendicectomy six to eight weeks later Approach B Immediate appendicectomy following inflammatory mass resolution Approach C An entirely conservative approach without interval appendicectomy in patients with appendiceal mass
APPENDICULAR MUCOCELE • Appendicular mucocele is a rare lesion (0.2 ‐ 0.3% of surgical appendicectomy specimens) • It is a descriptive term denoting an obstructive dilatation of the appendicular lumen by mucinous secretions
MUCINOUS CYSTADENOMA AND CYSTADENOCARCINOMA • MUCINOUS CYSTADENOMA AND CYSTADENOCARCINOMA ACCOUNT FOR 60 ‐ 70% OF ALL MUCOCELES • LESS COMMON CAUSES: • RETENTION CYST • MUCOSAL HYPERPLASIA • CARCINOID • APPENDICOLITH • ENDOMETRIOSIS • ADHESIONS • VOLVULUS
MUCINOUS CYSTADENOMA AND CYSTADENOCARCINOMA • ‐ High Correlation Of Synchronous Or Metachronous Colorectal • Adenomas And Carcinomas (Up To 20%) • ‐ Association With Mucin‐secreting Tumors Of The Ovary • ‐ PseudomyxomaPeritonei (Avoid Iatrogenic Rupture Of The Mucocele) • TREATMENT • Appendicectomy Is Used For Simple Mucocele Or For cystadenoma • Right Hemi‐colectomyIs Recommended For Cystadenocarcinoma
ILEO-PSOAS ABSCESS • Cough with expectorant,evening raise of temperature,haemoptysis, • Attitude of flexion,spinetenderness,gibbus • Cross fluctuation • No line of separation/space between mass&iliac spine
CROHN’S DISEASE • INFLAMMATORY DISEASE INVOLVING ILEUM , CAECUM , COLON • PTS.PRESENT WITH DIARRHOEA , FEVER , MULTIPLE FISTULA (PERIANAL) , WITH SIGNS OF INTESTINAL OBSTRUCTION • COBBLESTONE APPEARANCE , PSEUDOPOLYPS, SKIP LESIONS • STRING SIGN OF KANTOR ( NARROWING OF TERMINAL ILEUM )
ILEO-CAECAL TB ILEO CAECAL REGION IS MORE COMMONLY INVOLVED ??????? RICH LYMPHATICS IN PEYER’S PATCHES ALKALINE MEDIUM ILEOCECAL VALVE PRECIPITATES STASIS TERMINAL ILEUM IS MAXIMUM AREA OF RESORPTION
TREATMENT • CATEGORY I – ATT • IN CASE OF COMPLICATIONS • LIMITED RESSECTION • RIGHT HEMICHOLECTOMY
APPLE CORE APPEARANCE IN CA.CAECUM
RT.TUBO-OVARIAN MASS • Menstrual h/o; menorrhagia,polymenorrhagia,dysmenorrhea • Leucorrhea,dyspareunia, • Lower border not felt, • Per vaginal; rt.fornix tenderness,