Download
1 / 38
380 likes | 470 Views
Reducing Prenatal Alcohol Use: Effective Identification. Grace Chang, MD, MPH BFSS, San Francisco, CA 10 May 2006. Title Slide: Option 1A (with Harvard logo). Acknowledgements. National Institute on Alcohol Abuse and Alcoholism and Office of Research on Women’s Health* R01 AA 9670

E N D
Reducing Prenatal Alcohol Use:Effective Identification Grace Chang, MD, MPH BFSS, San Francisco, CA 10 May 2006
Acknowledgements • National Institute on Alcohol Abuse and Alcoholism and Office of Research on Women’s Health* • R01 AA 9670 • R01 AA 12548 • R01 AA 14678* • K24 AA 00289
Co-Investigators • E. John Orav, PhD • Susan Berman, MD • Louise Wilkins-Haug, MD, PhD • Research Team
2005 Advisory on Alcohol Use in Pregnancy • No amount of prenatal alcohol is safe • Alcohol can damage a fetus at any stage of pregnancy • Cognitive deficits and behavioral problems resulting from prenatal alcohol are lifelong • Alcohol related birth defects are entirely preventable
Prevalence of Prenatal Drinking • 13% of pregnant women drink • 40,000 babies with FASD annually • Lifetime cost per child is $860,000 • 6% with frequent (> 7 drinks/week) or binge (> 5drinks/episode) drinking • 21% prevalence in 1988 • Healthy People Goal • Achieving 6% prenatal drinking was the goal for 2000 • 6% is the goal for 2010
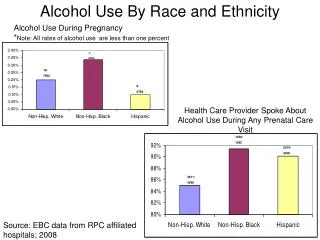
PRAMS Data, 2000-2001 • Pregnancy Risk Assessment Monitoring System identified women with the highest prevalence of alcohol use • Women > 35 years • Non-Hispanic Women • Women with > high school education • Women with higher incomes
Pregnant Binge Drinkers • Younger < 30 years • Single • White • Cigarette smoker • Uses illicit drugs • Marijuana (~20%), Cocaine (~11%), Other (~9%)
Fetal Alcohol Syndrome • With/without confirmed maternal alcohol exposure • Characteristic pattern of facial anomalies • Short palpebral fissures • Abnormalities of the premaxillary zone
Fetal Alcohol Syndrome • Growth retardation • Low birth weight, lack of weight gain over time, disproportional low weight to height • Neurodevelopmental CNS abnormalities • Small head size at birth • Structural brain abnormalities with age-appropriate neurological hard or soft signs (e.g., impaired fine motor skills)
Alcohol-Related Neurodevelopmental Disorder • One or more neurodevelopmental effects associated with fetal alcohol exposure • Alcohol-related problems • Behavior -Memory • Cognitive Function -Attachment • Fine motor skills -Language • Attention
Alcohol-Related Birth Defects • One or more birth defects associated with alcohol exposure • Cardiac (atrial septal defect, VSD) • Ocular (ptosis, corneal abnormalities) • Auditory (low-set posterior rotation of the auricle) • Renal (aplastic, hypoplastic, dysplastic) • Skeletal (fusion of radius and ulna)
Effects of One Drink • Growing evidence that prenatal alcohol consumption at levels < 1 drink/day can adversely affect fetal growth and development even in late pregnancy • “Ethanol inhibits neural cell adhesion” • “Mutations in cell adhesion molecule L1 cause mental retardation” • “Widespread apoptotic neurodegeneration” (deletion of millions of neurons, reduced brain mass)
One Drink per Week • Adverse effects evident in children at age 6 and 7 • Increased Aggressive and Externalizing Behavior • Dose response relationship • Increased Delinquent and Total Problem Behavior • Any prenatal alcohol exposure increased the risk of children (3.2 times) having Delinquent Behavior scores in the clinically significant range
Abstinence • Recommendation to preconceptional and pregnant women • American Academy of Pediatrics • American College of Obstetricians and Gynecologists • US Surgeon General • Secretary of Health and Human Services
Identification of Prenatal Alcohol Use • Increased ascertainment of alcohol use among periconceptional and pregnant women is urgently needed • Screening by obstetricians was 34% in 1987 and goal was 75% by 2000 • Special screening considerations
Identification Options • Standard Quantity and Frequency Questions • Many will alter drinking once pregnancy is confirmed • Denial and under-reporting for a multitude of reasons • Concurrent versus retrospective report of antenatal consumption
Current versus Retrospective Reports of Prenatal Alcohol Use • Jacobson et al. (‘91) found that 53% of the women who reported drinking more than 1.3 drinks/week while pregnant, recalled drinking more when interviewed after delivery • 42.1% drank more than 1.0 ounce of alcohol per day while pregnant
Breathalyzer or Urinalysis • Limited usefulness in the prenatal setting • Rapid metabolism of alcohol • Pattern of drinking by most pregnant women • Legal versus clinical procedure
Methods of Identification • Maternal Blood Markers • Combinations of MCV, GGT, CDT, WBAA (Whole Blood Acetaldehyde) for physically affected infants (Stoler et al., ‘98) • Neurobehavioral dysfunction (most frequent outcome) not recognized in the newborn period • Unlikely to be applicable to a substantial proportion of pregnant women • Harmful, but lesser amounts of consumption
Traditional Screening Instruments • Frequently developed among male drinkers • Limited utility in the prenatal setting • Brief questionnaires are most effective • Avoid triggering denial • Alcohol intake before pregnancy most important clinical predictor of subsequent use
Screening Instruments • Traditional screening instruments normed on male alcoholics (CAGE, SMAST) • Do not detect low but risky levels of drinking • Limitations among women and minorities • AUDIT • 10 items • Infrequently used • No established cut points for pregnant women
Other Options • AUDIT-C • Not well studied in prenatal populations • T-WEAK • Level of at-risk drinking detected is double the currently accepted level of a drink per day, (Sokol et al., 2003) • Low sensitivity as an alcohol screener among female veterans (Bust et al., 2003)
Sensitivity and Specificity: A Balance • Sensitivity • The probability that a person who should test positive, does so • Specificity • The probability that a person who should test negative, does so • More false positives versus more false negatives?
A Positive Screen • Not synonymous with an alcoholism diagnosis • Not an indictment • A signal for discussion • Appropriate balance between sensitivity and specificity
The T-ACE • Developed by Dr. R. J. Sokol • 4-item questionnaire based on the CAGE • Reflects a pattern of use • Validated in diverse patient samples • Detroit, MI and Boston, MA • Self-administered format in Boston
T-ACE Questions • T How many drinks does it take to make you feel high (effects)? • A Have people ever annoyed you by criticizing your drinking? • C Have you ever felt you ought to cut down on your drinking? • E Have you ever had a drink first thing in the morning to steady your nerves or get rid of a hang-over?
Scoring the T-ACE • T is given two points if the woman reports more than 2 drinks • A, C, E get one point each for each “yes” reply • T-ACE is positive with a score of 2 or more
Measures of Merit for the T-ACE • Superior to the AUDIT, MAST, Medical Record • Current Drinking • Risk Drinking • DSM-III-R Lifetime Alcohol Diagnoses • PAST drinking is most predictive of pregnancy drinking
T-ACE Positive Women • DSM-III-R criteria for lifetime alcohol dx • 40% + versus 14%T-ACE negative (p<.001) • Risk drinking pre-pregnancy (>2 drinks/ day) • 39% + versus 8% T-ACE negative (p<.001) • Drinking while pregnant • 43% + versus 13% T-ACE negative (p<.001)
T-ACE versus Medical Record • 278 pregnant women, all T-ACE positive • Electronic and paper obstetric records reviewed • 10.8% identified as potential drinkers • 82.2% of those who physicians did not consider to be at risk for alcohol use, drank • White women less likely to be identified by their doctors, even controlling for income, education, pre-pregnancy consumption (p=.026)
What to Do with a Positive T-ACE? • Discussion • Assessment • Brief Intervention
Recommendations • All pregnant women should be screened • Risk of prenatal alcohol use is not limited to the uneducated or impoverished • Use of a screening instrument will increase efficiency • Discussion, Assessment, or Brief Intervention • Highly therapeutic and effective in reducing drinking
References • Chang G, Wilkins-Haug L, Berman S, et al. Alcohol use and pregnancy: improving identification. Obstet Gynecol. 1998; 91: 892-8. • Chang G. Screening and brief intervention in prenatal care settings. Alcohol Research and Health. 2004/2005; 28: 80-84.