Download
1 / 30
300 likes | 309 Views
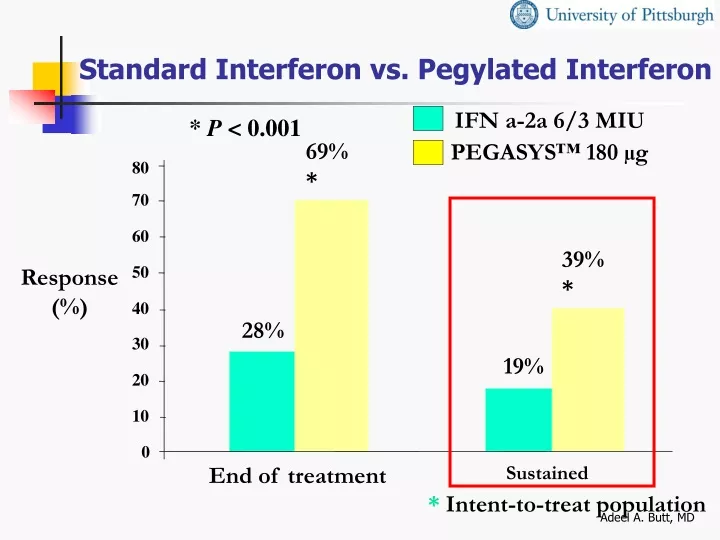
IFN a-2a 6/3 MIU. PEGASYS™ 180 µg. Standard Interferon vs. Pegylated Interferon. * P < 0.001. 69%*. 80. 70. 60. 39%*. Response (%). 50. 40. 28%. 30. 19%. 20. 10. 0. Sustained. End of treatment. * Intent-to-treat population. Standard Interferon vs. Pegylated Interferon.

E N D
IFN a-2a 6/3 MIU PEGASYS™ 180 µg Standard Interferon vs. Pegylated Interferon * P < 0.001 69%* 80 70 60 39%* Response(%) 50 40 28% 30 19% 20 10 0 Sustained End of treatment *Intent-to-treat population Adeel A. Butt, MD
Standard Interferon vs. Pegylated Interferon Genotype 1 40 28% 30 Patients with Response (%) 20 7% 10 0 IFN -2a PEG -IFN Zeuzem et al. NEJM 2000; 343:1666-1672 Adeel A. Butt, MD
Standard Interferon vs. Pegylated Interferon Genotype 2,3 56% 60 50 37% 40 Patients with Response (%) 30 20 10 0 IFN-2a PEG -IFN Zeuzem et al. NEJM 2000; 343:1666-1672 Adeel A. Butt, MD
PEG alone vs. IFN+RBV vs. PEG+RBV PEG-IFN -2a + Placebo (n = 224) IFN -2b + RBV (n = 444) PEG-IFN -2a + RBV (n = 453) Age (mean, y) 42.3 42.4 42.8 Male Gender68% 73% 71% Weight (kg) 78.9 78.1 79.6 Genotype 1 64% 64% 66% 2 and 3 31% 33% 31% HCV RNA Titers (mean, 106 c/mL) 5.9 6.0 6.1 Cirrhosis 15% 12% 12% Adeel A. Butt, MD Fried MW et al. NEJM 2002
PEG alone vs. IFN+RBV vs. PEG+RBVSustained Virologic Response P = 0.001 for all comparisons 56% 60% n = 453 45% 40% n = 444 30% % Patients n = 224 20% 0% IFN -2b + RBV PEG-IFN -2a + Placebo PEG-IFN -2a + RBV Adeel A. Butt, MD Fried MW et al. NEJM 2002
P = 0.001 P = 0.001 P = 0.001 P = 0.054 P = 0.016 P = 0.008 PEG alone vs. IFN+RBV vs. PEG+RBVSustained Virologic Response by Genotype 80 76% 70 61% 60 % of Patients 46% 45% 50 n = 140 37% 40 n = 298 n = 145 30 n = 69 21% n = 285 20 n = 145 10 0 Genotype 1 Genotype 2, 3 PEG-IFN -2a + PlaceboIFN -2b + RBV PEG-IFN -2a + RBV Adeel A. Butt, MD
IFN+RBV vs. Low Dose PEG+RBV vs. High Dose PEG+RBV 80 P = .01 P = .73 60 54 47 47 SVR (%) 40 20 (n = 505) (n = 514) (n = 511) 0 PEG (12 kDa) IFN alfa-2b1.5 / 0.5 g/kg+ RBV 1000-1200 mg PEG (12 kDa) IFN alfa-2b 1.5 g/kg+ RBV 800 mg IFN alfa-2b 3 MIU TIW + RBV 1000-1200 mg Adeel A. Butt, MD Manns et al. Lancet. 2001;358:958-965.
Flu-like symptoms Headache Fatigue or asthenia Myalgia, arthralgia Fever, chills Nausea Diarrhea Alopecia Thyroiditis Psychiatric symptoms Depression Mood lability Injection site reaction Autoimmunity Lab alterations Neutropenia Anemia Thrombocytopenia Side Effects of IFN Adeel A. Butt, MD
Side Effects of RBV • Hemolytic anemia • Teratogenicity • Cough and dyspnea • Rash and pruritus • Insomnia • Anorexia Rebetron [package insert]. Kenilworth, NJ: Schering Corp; 1999. Adeel A. Butt, MD
PEG (12 kDa) IFN alfa-2b Incidence of Discontinuations Due to Adverse Events 14 13 13 14 12 10 8 Percent 6 4 2 0 IFN alfa-2b + RBV PEG IFN alfa-2b (12 kDa) 1.5 µg/kg + RBV PEG IFN alfa-2b (12 kDa) 1.5/0.5 µg/kg + RBV Adeel A. Butt, MD IFN = interferon; PEG = polyethylene glycol; RBV = ribavirin.
HCV and HIV - Similarities HCV HIV • + ssRNA – Flavivirus • Virions/d = 1012 • Diversity/complexity • Six genotypes • Tropism: hepatocyte • Receptors: LDL, CD81 • + ssRNA – Retrovirus • Virions/d = 1010 - 1011 • Diversity/complexity • 11+ clades • Tropism: lymphoid • Receptors: CD4, CCR5 HIV CCR5 = chemokine receptor 5; CD4 = cluster of deviation 4; CD81 = cluster of deviation 81; LDL = low density lipoprotein; + ssRNA = positive single strand ribonucleic acid. Adeel A. Butt, MD
HCV and HIV • Prevalence of HCV in HIV > 10x general population • Reported to be between 30-50% • ~6% of VA population HCV infected • ~35-43% of HIV infected veterans have HCV Greub, Lancet 2000;356:1800-5 Adeel A. Butt, MD
Hepatitis C Virus and HIV Liver-Related Mortality • UK hemophilia population, 1985-1998 • Deaths due to liver disease • HIV - 16.7-fold • HIV + 94.4-fold • Risk after 10 years 80 60 Deaths Due to Liver Disease (O/E) 40 20 0 HIV+ HIV- GP GP = general population; HIV = human immunodeficiency virus; O/E = observed to expected. Adeel A. Butt, MD
Increasing Mortality From ESLD in Patients With HIV • One third of 1998 cohort had recent history of discontinuing HAART secondary to hepatotoxicity • More than 1/2 who died with ESLD had either NDVL or CD4 >200/mm3 6 months prior to death 50 40 30 20 10 0 50 1991 1996 1998 ESLD-Related Deaths (%) 14 11 ESLD = end stage liver disease; NDVL = no detectable viral load. Adeel A. Butt, MD
HCV-HIV Co-infection • Progression of liver disease accelerated in HCV-HIV co-infected patients • Median time to cirrhosis 7 years in HCV-HIV vs. 23 years in HCV alone Adeel A. Butt, MD Soto, J Hepatol 1997;26:1-5
Generally no increase in HIV progression No difference in survival, progression from HIV to AIDS or AIDS to death or HIV to death Rate of decline of CD4 counts is also similar Dorrucci, JID 1995;172:1503-8 Staples Clin Infect Dis 1998;29:150-4 Sulkowski JAMA 2002 More AIDS at baseline More progression Decreased CD4 recovery Greub, Lancet 2002 De Luca, Archives 2002 HCV-HIV Co-infection Effect of HCV on HIV Progression CONTROVERSIAL Adeel A. Butt, MD
PEG-IFN + RBV is associated with a superior week 24 virologic response (VR) IFN + RPEGIFN + R n=67 n=66p value Overall Wk 24 VR* 10 (15%) 29 (44%) 0.0003 genotype 1** 4/52 (7%) 17/51 (33%) 0.0014 genotype non-1** 6/15 (40%) 12/15 (80%) 0.06 biochemical response 44% 54% NS *intent to treat **Genotype 1 vs. non-1, p < 0.0001 Slide courtesy of R. Chung Adeel A. Butt, MD
A significant portion of virologic nonresponders experience histologic response (HR) IFN + RPEGIFN + R n=67 n=66 p value Virologic nonresponders 57 (85%) 37 (56%) 0.0003 Wk 24 Bx obtained 37 23 Histologic response 15 (40%) 6 (26%) 0.28 Combined virologic and histologic response VR + HR 25 (37%) 35 (53%) 0.08 Slide courtesy of R. Chung Adeel A. Butt, MD
Grade 4 events IFN + R PEGIFN + R n = 67 n = 66 p value • Grade 0-1 18 9 NS • Grade 2 25 18 NS • Grade 3 20 22 NS • Grade 4 4 17 0.0012 • ANC (< 500) 3 7 NS • gluc (> 500) 0 4 NS • plt (< 20K) 0 1 NS • LFTs (> 10x ULN) 0 2 NS • depression 1 0 NS • Premature D/C 8 (12%) 8 (12%) NS Adeel A. Butt, MD Slide courtesy of R. Chung
Absolute CD4 fell but CD4% rose IFN + RPEGIFN + R p value Wk 0 CD4 452 500 0.07 %CD4 24.0 25.5 0.19 Wk 24 CD4 369 363 0.80 %CD4 27.0 30.5 0.10 DCD4 W0-24 -112 -194 0.01 D%CD4 W0-24* +2.5% +3.5% 0.14 *overall +3.0%, p = 0.0001 Slide courtesy of R. Chung Adeel A. Butt, MD
There was no adverse effect on HIV-1 control HIV RNA Total IFN + RPEGIFN + Rn = 119n = 62 n = 57p W0 W24 und und 59 (50%) 32 (52%) 27 (47%) NS und det 9 (8%) 6 (10%) 3 (5%) NS det und 16 (13%) 6 (10%) 10 (5%) NS det det 35 (29%) 18 (29%) 17 (30%) NS W0 undetectable 38 (62%) 30 (52%) NS W24 undetectable 38 (62%) 37 (65%) NS Slide courtesy of R. Chung Adeel A. Butt, MD
HCV-HIV Co-infected Patients • 51 patients • IFN alfa 2b, 3 million units TIW PLUS RBV 1000-1200 • 12 months • 59% genotype 1 • Cirrhosis – 55% • Mean CD4 = 411 Landau. AIDS 2001;15:2149-2155. Adeel A. Butt, MD
HCV-HIV Co-infected Patients • ETVR = 29% • SVR = 21% • CD4 drop at end of treatment = 51 normalized after 6 months • Treatment discontinuation 29% Landau. AIDS 2001;15:2149-2155. Adeel A. Butt, MD
Hepatotoxicity in Co-infected Patients • May be more common in co-infected patients, esp. those on PI based regimens • However, overall risk small • 88% co-infected patients on HAART had NO toxicity • Reversible in those in whom it occurred • Difficult to provide guidelines on management: • Stop or change therapy if liver enzymes > 3-5 times ULN Sulkowski, JAMA 2000;283:74-80. Adeel A. Butt, MD
Managing Depression • Take psychiatric history for depression and mania • Develop relationship with mental health providers • Treat preexisting depression before starting (PEG) IFN • Evaluate patients for development of depression at least every 2 weeks after initiation of IFN therapy • Mild depression – evaluate weekly • Moderate depression – reduce dose of IFN; consider psychiatric consultation • PEG IFN alfa-2a: reduce to 135 µg weekly • PEG IFN alfa-2b: reduce dose by 1/2 • Severe depression – discontinue IFN/RBV immediately and permanently; obtain immediate psychiatric consult Adeel A. Butt, MD
Management of Neutropenia • Neutropenia • Consider G-CSF 300 µg SC BIW or TIW • No controlled trials demonstrating effectiveness • Clinical experience shows this to be effective • ANC <750 cells/mm3– dose reduce IFN • PEG IFN alfa-2a: decrease to 135 µg weekly • PEG IFN alfa-2b: decrease dose by 1/2 • ANC <500 cells/mm3– discontinue IFN Adeel A. Butt, MD GCSF = granulocyte-colony stimulating factor.
Management of RBV-Induced Anemia • Hemoglobin determinations pretreatment, at week 2, week 4, and as needed • If >10 g/dL: no action needed • If <10 g/dL: reduce RBV dose to 600 mg daily • If <8.5 g/dL: stop RBV • If decreases by >2 g/dL from starting therapy:reduce dose to 600 mg daily in patients with cardiac history • Hemoglobin returns to baseline within 4 weeks after RBV is stopped • Cardiac function • Anemia may exacerbate symptoms of coronary disease and/or deteriorate cardiac function • Recommend stress test for patients aged >50 years • Consider epoetin alfa 40,000 IU SC QW Adeel A. Butt, MD
Conclusions • HCV is a common disease and a frequent cause of morbidity and mortality in the US and globally • Current treatment options can eradicate/cure HCV in a significant proportion of chronically infected patients • Very few eligible patients actually receive treatment • HCV co-infection is very common in the HIV infected patients • Treatment is associated with significant adverse events, especially in the HCV-HIV co-infected patients • Benefits of treatment should be weighed against the risks, considering the long natural history of the disease Adeel A. Butt, MD