Download
1 / 16
290 likes | 789 Views
A review by Lindsey Tucker, MD. Phantom Limb Pain. Incidence. An estimated 1.7 million people in the US are living with limb loss. Each year 158,000 persons undergo an amputation The incidence of phantom pain is 60-80% among amputees.

E N D
A review by Lindsey Tucker, MD Phantom Limb Pain
Incidence • An estimated 1.7 million people in the US are living with limb loss. • Each year 158,000 persons undergo an amputation • The incidence of phantom pain is 60-80% among amputees. • Independent of adult age, gender or location or side of amputation (less common in children or congenital amputees)
Onset and Duration • Several studies have shown that 75% of patients with PLP develop pain within the first few days after amputation. • One study of 58 amputees found incidence of PLP to be 72%, 65% and 59% after 1 week, 6 months and 2 years. (Jensen, et al 1985) • Another study of 56 amputees showed that although the incidence and intensity of pain remained constant, the frequency and duration of pain attacks decreased significantly. (Nikolajsen, et al 1997)
Character and association • Phantom pain is usually intermittent; only few patient’s are in constant pain. • Pain is primarily located in distal parts of the missing limb. • Few case reports suggest that pre-amputation pain may persist as PLP, but this is not the case in most patients. • Phantom pain is more frequent in patients with long-term stump pain, and decreases with resolution of stump-end pathology
Mechanisms of Phantom Pain • Following a nerve cut, formation of neuromas are seen, which show spontaneous and abnormal evoked activity following mechanical and chemical stimulation. (Amir, et al 1993) • Percussion of stump/neuromas induces stump and PLP; increased activity of afferent C fibers (Nystrom, et al 1981) • Perineuromal injection of gallamine produces PLP, injection of lidocaine blocks PLP. (Chabal, et al 1981)
Spinal Plasticity • After nerve injury, C-fibers and A delta-afferents gain access to secondary pain signaling neurons (mediated by glutamate and neurokinins). This is manifested by mechanical hyperalgesia and expansion of peripheral receptive fields. (Doubell, et al 1999) • Increased activity of NMDA receptor; central sensitization can be reduced by NMDA antagonists such as ketamine. (Eichenberger, et al 2008)
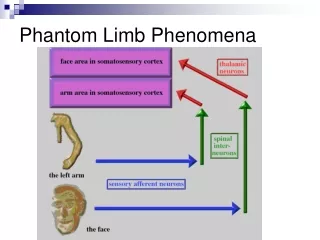
Anatomical reorganization • Peripheral nerve damage can lead to degeneration of C-fiber afferent terminals in laminae II. As a result, central terminals of Aβ-mechanoreceptive afferents (which normally terminate in laminae III and IV) sprout into laminae I and II. (Woolf, et al 1992) • Ultimately, this results in increased general excitability of spinal cord neurons.
Sympathetic nervous system role • Application of norepinephrine or activation of post-ganglionic sympathetic fibers excites and sensitizes damaged (not normal) nerve fibers. (Devor, et al 1994) • Sympatholytic block can abolish neuropathic pain, but pain can be rekindled by injection of norepinephrine under the skin. (Torebjork et al 1995)
Cerebral reorganization • One study of adult monkeys revealed cortical reorganization in which the mouth and chin invade cortices corresponding to arm and digits. (Dotrovsky, et al 1999) • In humans, similar reorganization has been observed using magnetoencephalographic techniques and there was a linear relationship between pain and degree of reorganization (flor, et al 1998)
Medication trials • TCA’s and sodium channel blockers are currently considered the drug treatments of choice for neuropathic pain, but a 2004 study of 39 patients demonstrated no benefit of TCA’s over placebo in PLP after 6 weeks. (Robinson et al 2004) • One study showed that mexiletine produced pain relief in 18 of 31 patients with PLP. (Davis 1993) • Opioids (MST) produced pain relief in 42% of patients and showed evidence of reduced cortical reorganization in 12 patients with PLP. (Huse E 2001) • There have been mixed results in studies using memantine to treat chronic pain, but it may be successful in treating PLP if initiated in early post-amputation period. (Hackworth, et al 2008)
Adjuvant therapies • TENS has reduced PLP in multiple placebo controlled trials. • Mirror box therapy: persons with amputated limb use either a mirror or mirror box to reflect an image of the intact limb. It is hypothesized that this works by preventing cortical restructuring. • One RCT of 22 patients showed 100% of patients with MBT showed decreased pain after 4 weeks. (Chan BL 2007)
Prevention • It was hypothesized that pre-amputation pain created an imprint in the CNS such that it could cause pain after the amputation. • Studies are mixed, but some show that the incidence of PLP is decreased at 6 and 12 months if an epidural is placed pre-operatively and continued 3-7 days post-op.