Download
1 / 46
770 likes | 3.28k Views
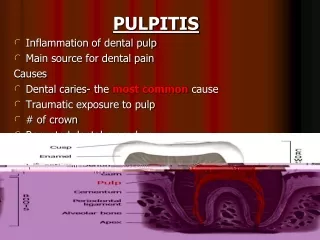
Open Pulpitis. By : Mohammed El-Said Abu El-Naga Oral and Maxillofacial Surgery. CLASSIFICATION OF PULPITIS. Chronic open pulpitis. The extension of a carious lesion or trauma may result in a connection between the oral cavity and the pulp tissue. Ulcerative open chronic pulpitis.

E N D
Open Pulpitis By : Mohammed El-Said Abu El-Naga Oral and Maxillofacial Surgery By:Dr/M.Abuelnaga
CLASSIFICATION OF PULPITIS By:Dr/M.Abuelnaga
Chronic open pulpitis. The extension of a carious lesion or trauma may result in a connection between the oral cavity and the pulp tissue . By:Dr/M.Abuelnaga
Ulcerative open chronic pulpitis Ulcerative open chronic pulpitis is associated with an ulcerative pulp surface in the area of exposure of the pulp cavity, ie healing prospects are poorer in this area. The pulp tissue lying beneath this surface either presents as a diffuse chronic inflammation or merely shows signs of hyperaemia. By:Dr/M.Abuelnaga
Clinically Chronic ulcerative pulpitis sharp probes have to wear marrow cavities deep exploration hole, a moderate degree of exploration can be painful; diagnosis or electric hot and cold reaction diagnosis can be slow or sensitive; percussion may have mild discomfort. By:Dr/M.Abuelnaga
X-rays examination may have the periodontal ligament space widened periapical plate blurred or hard to change. By:Dr/M.Abuelnaga
Granulomatous open chronic pulpitis(pulp polyp) If the blood supply is sufficient, open chronic pulpitis can change to granulomatous open chronic pulpitis (pulp polyp). Granulation tissue sprouts from the ulcerative surface tissue and slowly grows to an enlarging mass of tissue from the pulp cavity through the opening of the pulp roof into the oral cavity. By:Dr/M.Abuelnaga
Pulp polyp By:Dr/M.Abuelnaga
Pulp polyp By:Dr/M.Abuelnaga
History Pulp polyps are usually asymptomatic . Direct pressure during mastication may cause mild-to-moderate tenderness . Localized bleeding may occur when the soft tissue is manipulated or traumatized . All lesions are associated with a history of a long-standing carious lesion, a fractured tooth due to trauma, or a combination or these 2 insults . By:Dr/M.Abuelnaga
Pulp polyps reach a maximum size within a couple of months and then remain static . Mobility of the tooth and sensitivity to percussion are usually absent . Drainage of a purulent exudate is not a characteristic finding . By:Dr/M.Abuelnaga
Physical A spongy, soft tissue nodule extrudes from the cavitated or fractured surface of a tooth . The surface varies from pink and smooth to red and white and granular . Polyps typically enlarge to fill the entire cavitated area or pulpal chamber of the tooth . Soft tissue may merge with the adjacent attached gingiva . Polyps usually develop in carious primary molars and first permanent molars because, anatomically in young persons, these teeth have large pulp chambers. By:Dr/M.Abuelnaga
Less frequently, maxillary central incisors in both dentitions are affected . A pulp polyp is a single lesion, but multiple teeth may be affected . Teeth with open or incomplete apexification of the root apices are the most susceptible . Extrusion of the opposing molar or tipping of the adjacent teeth with space loss may be observed when significant destruction of the crown occurs . By:Dr/M.Abuelnaga
Causes Causes of a pulp polyp include the following : Carious tooth with significant loss of tooth structure . Loss of a dental restoration that results in pulpal exposure . Fractured tooth due to trauma with a pulpal exposure . Pulpal tissue with access to a good blood supply . Possible hormonal (estrogen and progesterone) influence . By:Dr/M.Abuelnaga
Differential Diagnoses Pyogenic Granuloma (Lobular Capillary Hemangioma ) By:Dr/M.Abuelnaga
Imaging Studies Intraoral radiographs, in particular periapical and bite-wing film views, are needed to confirm this diagnosis and to determine the extent of tooth destruction and if the inflammatory lesion involves the surrounding alveolar bone . Radiographic findings demonstrate a large coronal radiolucency that extends to the pulpal chamber with focal loss of tooth structure, while the root apices may be either open or closed . Although no bony changes are usually observed, the surrounding alveolar bone may reveal either an incipient periapical radiolucency that is consistent with chronic apical periodontitis or a localized radiopacity that is referred to as focal sclerosing osteomyelitis (condensing osteitis). By:Dr/M.Abuelnaga
In addition, vertical alveolar bone height may be decreased surrounding the involved tooth, which is indicative of periodontitis . Radiographic imaging is required to determine the most appropriate treatment for the involved tooth . By:Dr/M.Abuelnaga
Pulp polyp radiographically By:Dr/M.Abuelnaga
Other Tests Diagnosis and determination of the most appropriate treatment options are based on adjunctive tests, including response to percussion, thermal stimuli, and electric pulp testing. In most cases, the results of these adjunctive tests are similar to those obtained for healthy teeth, which is in contrast to most teeth that exhibit irreversible pulpitis. By:Dr/M.Abuelnaga
Electrical pulp tester By:Dr/M.Abuelnaga
The normal responses should not confuse the practitioner that the pulpal tissue is healthy and therefore requires only conservative treatment. In addition, these tests help to differentiate a true pulp polyp from hyperplastic gingivitis that is overlying a cavitation from a nonvital tooth . By:Dr/M.Abuelnaga
Correlation between Pulp Vitality & Chronic Open Pulpitis Examination of human non-epitheliated and epitheliated pulp polyps, using paraffin sections stained with Holmes' silver stain, showed nerve fibers present in the connective tissue of the pedicle region, in the granulation tissue of the polyp, and in the epithelium. By:Dr/M.Abuelnaga
A similar innervation was present in some of the epitheliated polyps to that described in the oral mucosa. Pulp nerves never innervate epithelium under normal circumstances, so that the innervation of epithelium covering a pulp polyp is a unique example of innervation of a newly formed mature tissue after fetal life (Southam et al, 1973). By:Dr/M.Abuelnaga
An electron microscope study of ultra-thin sections of hypertrophic pulps removed from human teeth showed that the epithelial cells which covered the oral surface of the polyps were closely related to one another by “intercellular bridges” and desmosomes. Structures resembling half desmosomes attached the epithelial cells to the underlying basement membrane and were a prominent feature of the scalloped boundary zone between epithelial and connective tissue elements . By:Dr/M.Abuelnaga
Although somatic myelinated nerve fibres were not seen, small bundles of unmyelinated nerve fibres were observed in the connective tissue of the polyps (Dixon et al, 1965). Chronic inflammation is often associated with irreversible destruction of parenchymal tissue, and fibrous connective tissue fills the resultant defect. Proliferation of fibroblasts, collagen production, and neovascularization are enhanced by the secretion of cytokines by T cells and macrophages. It may be concluded that epithelium of pulp polyps show morphologic characteristics similar to the epithelium of oral mucosa . The connective tissue shows characteristics of chronic inflammation of varied intensity (Trowbridge, 1990). By:Dr/M.Abuelnaga
Presumably the young pulp does not become necrotic following exposure, because its natural defenses and rich supply of blood allow it to resist bacterial infection. Transudates and exudates which are inflammatory response products in open chronic pulpitis, drain into the oral cavity and do not accumulate. Thus intra-pulpal pressure, which may consequently cause tissue damage and destruction of the microcirculation, does not develop (Faryabi & Adhami, 2008). By:Dr/M.Abuelnaga
Histologic Findings Microscopic findings reveal a mass of granulation tissue protruding from the crown of a fractured or carious tooth that resembles a pyogenic granuloma. The fibrovascular stroma contains numerous small, delicate vascular channels and a prominent inflammatory infiltrate composed of primarily lymphocytes, plasma cells, and neutrophils. Although the surface may be ulcerated, it is covered by stratified squamous epithelium that resembles oral mucosa in approximately 50% of these inflammatory hyperplastic lesions. By:Dr/M.Abuelnaga
The source of this epithelium appears to be from the engraftment of desquamated oral epithelial cells or the migration of the epithelium from the adjacent gingival tissues. In more mature lesions that are covered with squamous epithelium, the granulation tissue is replaced by fibrous connective tissue with minimal inflammation and foci of dystrophic calcification . By:Dr/M.Abuelnaga
Bacteria (primarily gram positive) are found on the surface of the polyp and within the carious lesion. In many cases, the histopathologic changes are limited to the coronal pulp tissue with the apical tissue exhibiting only mild vasodilation and minimal chronic inflammation . Ultrastructural examination of nerve fibers associated with the pulp polyp exhibits variable findings within the same tooth, ranging from normal to moderate or severe degeneration of both myelinated nerve fibers and unmyelinated nerve fibers .. By:Dr/M.Abuelnaga
pulp polyp histologically By:Dr/M.Abuelnaga
Treatment Medical Care Treatment of a pulp polyp in a permanent tooth includes either root canal therapy or extraction of the tooth . The more conservative pulpotomy treatment has been successful in selected cases when only the coronal pulp is affectedIn immature teeth with incomplete root development, placement of an apical barrier and strengthening of the thin root with composite resin may be indicated prior to root canal treatment . By:Dr/M.Abuelnaga
Pulp revascularization of an immature permanent tooth is another new treatment approach that results in the formation of vital pulpal tissue . The tooth requires a full-coverage crown following endodontic therapy . By:Dr/M.Abuelnaga
Surgical Care The affected tooth is extracted when primary teeth are involved or when minimal tooth structure in permanent teeth is available for restoration or the alveolar bone support is unfavorable . A surgical crown lengthening procedure may be needed to prepare a tooth for a full-coverage crown . Healing is uneventful in most cases . By:Dr/M.Abuelnaga
Medication Systemic medications are not recommended for the management of this lesion. Antibiotics are not prescribed for the treatment of the pulp polyp, despite a bacterial component. However, an antibiotic paste mixture is used within the canals of the infected tooth when the revascularization process is performed for the treatment of the nonvital tooth . By:Dr/M.Abuelnaga
Further Outpatient Care Periodic dental examinations are recommended to monitor the success of the root canal therapy or to intercept problems associated with the premature loss of a tooth . Orthodontic treatment may be needed to restore the occlusion . If a tooth is extracted, either a dental implant or fixed dental prosthesis (bridge) is a treatment option to restore function and aesthetics . By:Dr/M.Abuelnaga
Complications Space discrepancy from crown destruction or premature loss of a tooth may result in a crowded malocclusion, supereruption of an opposing tooth, or the impaction of a succedaneous tooth . Without definitive treatment, some of these long-standing, nonvital teeth may progress to symptomatic disease, including periapical inflammatory disease and (rarely) cellulitis and osteomyelitis of the jaws . By:Dr/M.Abuelnaga
Prognosis The prognosis is excellent. No risk for recurrence exists once definitive treatment has been rendered . By:Dr/M.Abuelnaga
Patient Education Reinforce the importance of routine oral health care to prevent the development of deep carious lesions that may cause inflammatory pulpal disease and more serious sequelae . By:Dr/M.Abuelnaga
Histological evaluation of teeth with hyperplastic pulpitis caused by trauma or caries: case reports AIM The purpose of this histological study was to examine teeth with hyperplastic pulpitis caused by trauma or caries. SUMMARY The pulp tissue of one young permanent incisor with a complicated crown-root fracture and a hyperplastic pulpitis, which had been contaminated with oral microflora for 40 days, and pulp polyps from four permanent first molars whose crowns were destroyed by extensive caries were prepared for standard histological examination. By:Dr/M.Abuelnaga
Histologically, Normal pulp tissue organization was observed in the tooth with a complicated crown-root fracture in the cervical radicular region. Irregular calcification was seen in the coronal and radicular portion of the pulp in the four carious teeth with pulp polyps. Radicular pulp tissue in the middle and apical third of root canals beneath irregular calcification showed intensive fibrosis but was free from inflammatory cells. By:Dr/M.Abuelnaga
KEY LEARNING POINTS Hyperplastic pulpitis is a type of irreversible chronic open pulpitis. Young permanent teeth with hyperplastic pulpitis caused by trauma or caries have a great inherent defensive capacity to heal. By:Dr/M.Abuelnaga
Pulp polyp associated with a natal tooth: case report Natal teeth are an infrequent occurrence at birth. Often these teeth are extracted because they are very mobile and pose a risk of aspiration. This is a rare case in which a natal tooth was extracted by the pediatrician with his fingers. A root fragment remained and out of this developed a large pulp polyp. This relationship has not been previously reported . By:Dr/M.Abuelnaga
References Catherine M, Jan 23, 2012 Pulp Polyp Clinical Presentation. Medscape Reference Assem M, Jan 2012 Correlation between Pulp Vitality & Chronic Open Pulpitis. PathXchange / Global Online Pathology Community Calişkan M.K, Oztop F, Calişkan G, 2003 Jan, Histological evaluation of teeth with hyperplastic pulpitis caused by trauma or caries: case reports. Endod J.; 36 (1):64-70 Vergotine R, Hodgson B, Lambert L, 2010 Pulp polyp associated with a natal tooth: case report. J Clin Pediatr Dent.; 34 (2):161-3 By:Dr/M.Abuelnaga
Thank You By:Dr/M.Abuelnaga