Download
1 / 1
10 likes | 77 Views
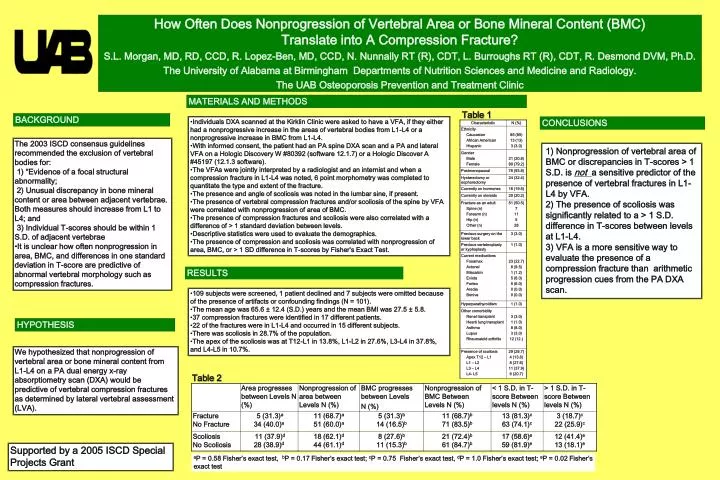
How Often Does Nonprogression of Vertebral Area or Bone Mineral Content (BMC) Translate into A Compression Fracture? S.L. Morgan, MD, RD, CCD, R. Lopez-Ben, MD, CCD, N. Nunnally RT (R), CDT, L. Burroughs RT (R), CDT, R. Desmond DVM, Ph.D.

E N D
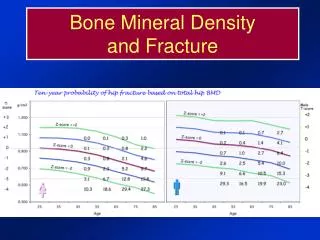
How Often Does Nonprogression of Vertebral Area or Bone Mineral Content (BMC) Translate into A Compression Fracture? S.L. Morgan, MD, RD, CCD, R. Lopez-Ben, MD, CCD, N. Nunnally RT (R), CDT, L. Burroughs RT (R), CDT, R. Desmond DVM, Ph.D. The University of Alabama at Birmingham Departments of Nutrition Sciences and Medicine and Radiology. The UAB Osteoporosis Prevention and Treatment Clinic MATERIALS AND METHODS Table 1 BACKGROUND • Individuals DXA scanned at the Kirklin Clinic were asked to have a VFA, if they either had a nonprogressive increase in the areas of vertebral bodies from L1-L4 or a nonprogressive increase in BMC from L1-L4. • With informed consent, the patient had an PA spine DXA scan and a PA and lateral VFA on a Hologic Discovery W #80392 (software 12.1.7) or a Hologic Discover A #45197 (12.1.3 software). • The VFAs were jointly interpreted by a radiologist and an internist and when a compression fracture in L1-L4 was noted, 6 point morphometry was completed to quantitate the type and extent of the fracture. • The presence and angle of scoliosis was noted in the lumbar sine, if present. • The presence of vertebral compression fractures and/or scoliosis of the spine by VFA were correlated with nonprogression of area of BMC. • The presence of compression fractures and scoliosis were also correlated with a difference of > 1 standard deviation between levels. • Descriptive statistics were used to evaluate the demographics. • The presence of compression and scoliosis was correlated with nonprogression of area, BMC, or > 1 SD difference in T-scores by Fisher’s Exact Test. CONCLUSIONS • The 2003 ISCD consensus guidelines recommended the exclusion of vertebral bodies for: • 1) “Evidence of a focal structural abnormality; • 2) Unusual discrepancy in bone mineral content or area between adjacent vertebrae. Both measures should increase from L1 to L4; and • 3) Individual T-scores should be within 1 S.D. of adjacent vertebrae • It is unclear how often nonprogression in area, BMC, and differences in one standard deviation in T-score are predictive of abnormal vertebral morphology such as compression fractures. 1) Nonprogression of vertebral area of BMC or discrepancies in T-scores > 1 S.D. is not a sensitive predictor of the presence of vertebral fractures in L1- L4 by VFA. 2) The presence of scoliosis was significantly related to a > 1 S.D. difference in T-scores between levels at L1-L4. 3) VFA is a more sensitive way to evaluate the presence of a compression fracture than arithmetic progression cues from the PA DXA scan. RESULTS • 109 subjects were screened, 1 patient declined and 7 subjects were omitted because of the presence of artifacts or confounding findings (N = 101). • The mean age was 65.6 ± 12.4 (S.D.) years and the mean BMI was 27.5 ± 5.8. • 37 compression fractures were identified in 17 different patients. • 22 of the fractures were in L1-L4 and occurred in 15 different subjects. • There was scoliosis in 28.7% of the population. • The apex of the scoliosis was at T12-L1 in 13.8%, L1-L2 in 27.6%, L3-L4 in 37.8%, and L4-L5 in 10.7%. HYPOTHESIS We hypothesized that nonprogression of vertebral area or bone mineral content from L1-L4 on a PA dual energy x-ray absorptiometry scan (DXA) would be predictive of vertebral compression fractures as determined by lateral vertebral assessment (LVA). Table 2 Supported by a 2005 ISCD Special Projects Grant aP = 0.58 Fisher’s exact test, bP = 0.17 Fisher’s exact test; cP = 0.75 Fisher’s exact test, dP = 1.0 Fisher’s exact test; eP = 0.02 Fisher’s exact test