Download
1 / 43
490 likes | 1.02k Views
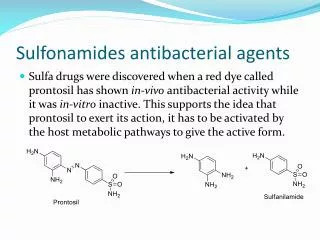
SULFONAMIDES. First effective chemotherapeutic agent. Chemistry. Structural analogue of PABA . Sulfonamides are with diff. chemical, physical, pharmacological and anti bacterial properties.

E N D
SULFONAMIDES First effective chemotherapeutic agent
Chemistry • Structural analogue of PABA. • Sulfonamides are with diff. chemical, physical, pharmacological and anti bacterial properties. • Produced by substitutions at gp (-SO2 –NH –R) or the amide group (-NH2) of sulfanilamide nucleus. • Sulfanilamide is para-aminobenzenesulfonamide
CLASSIFICATION • Well absorbed by Mouth and Rapidly eliminated (short Acting) a. General Purpose • Sulfadiazine b. Mainly for UTI • Sulfisoxazole • Sulphamethizole • Sulfamethoxazole
Well absorbed by GIT and Slowly eliminated (Long Acting) • Sulphadoxine • Sulphamethoxypyridazine • Sulphadimethoxine • Sulphaphenazole • Poorly absorbed by GIT • Sulfasalazine
For Topical Application • Sulfacetamide • Silver Sulfadiazine • Mafenide • Miscellaneous Group Sulfapyridine • Sulfonamide Combination • Cotrimoxazole (Sulfamethoxazole & trimethoprim) • Fansidar (Sulfadoxine & Pyrimethamine)
PHARMACOKINETICS Mostly well absorbed after oral adm. Divided into three major groups. • Oral absorbable • Oral non absorbable • Topical
Oral absorbable absorption – stomach and intestine Distribution – Widely distributed CNS, CSF, placenta and fetus PPB 20 – 90 % to serum albumin PPL 2 – 6 hrs Metabolism – Liver Excretion – Urine , feces, bile, milk and other secretions
Metabolism • A portion of the absorbed drug is acetylated or glucronidated in the liver. • Dosage reduction is required in renal failure.
PABA MOA They are bacteriostatic X Dihydropteroate Synthase Sulfonamides Dihydrofolic Acid (Folate) X Dihydrofolate Reductase Trimethoprim Tetrahydrofolic Acid Purines DNA
Sulfonamides susceptible organisms, unlike mammals, cannot use exogenous folate but must synthesize it from PABA.
ANTIBACTERIAL SPECTRUM • Exert bacteriostatic effect • Gram +veand Gram -ve bacteria • Some enteric bacteria like E. Coli, Shigella, Salmonella, Klebsiella. • Nocardia, Chlamydia trachomatis and some protozoa.
Resistance • Mammalian cells lack the enzymes required for folate synthesis from PABA and depend on exogenous source of folate, so they are not susceptible to sulfonamides.
Resistance in bacteria • Sulfonamides resistance may occur as a result of mutations. • A- Overproduction of PABA • B- Production of a folic acid synthesizing enzyme that has low affinity for sulfonamides. • C- Impair permeability to the sulfonamideor active efflux • An alternative metabolic pathway for synthesis of essential metabolite
Therapeutic Uses • A- Oral Absorbable Agents Urinary Tract Infections Not therapy of first choice Sulfadiazine with pyrimeythamine---acute toxoplasmosis • B- Oral Nonabsorbable Agents Sulfasalazine is used in ulcerative collitis, enteritis and other inflammatory bowl disease.
C- Topical Agents Sodium sulfacetamide ophthalmic solution or ointment is used for Bacterial conjunctivitis Trachoma Silver sulfadiazine used for prevention of infection of burn wounds.
Nocardiosis: Sulfisoxazoleor sulfadiazine
Used in combination • Pneumocystis Carinii – sulfamethoxazole combined with trimethoprim (Co-trimoxazole) • Resistant Malaria (Sulfadoxine + Pyrimethamine – Fansidar) • Acute toxoplasmosis – (Sulfadiazine + Pyrimethamine)
ADVERSE EFFECTS • Hypersensitivity Reactions:- 1. Fever, Skin rashes, exfoliative dermatitis, photosensitivity, urticaria, N, V, D Angioedema & Steven – Johnson syndrome Stomatitis, conjunctivitis, arthritis and hepatitis. 2.Hematopoietic Disturbances :- Hemolytic or Aplastic anemia, Granulocytopenia, Thrombocytopenia, Leukemoid reactions Can provoke hemolytic reactions in patients with glucose-6-phosphate dehydrogenase deficiency.
Urinary Tract Disturbances:- Sulfonamides may precipitate in urine, especially at neutral or acid pH producing crystalluria, Hematuria or even obstruction and nephritis Less with sulfisoxazole. • Treatment Sodium bicarbonate and adequate hydration.
CONTRAINDICATIONS • Premature babies, newborns & infants less than 2 months • Pregnant woman at term – Kernicterus • Displacement of bilirubin from plasma albumin. • Deposition of bilirubin in basal ganglia and sub thalamic nuclei of brain.
Drug interactions • Oral anticoagulants • Sulfonylurea • Hydantoin anticonvulsants • Potentiate the effect of these drugs • Inhibition of metabolism or displacement from albumin
TRIMETHOPRIM Chemistry: Trimethoxybenzyl Pyrimidine Chemically Related to anti malarial drug pyrimethamine both are folate antagonists.
MOA PABA X Dihydropteroate Synthetase Sulfonamides Dihydrofolic Acid (Folate) X Dihydrofolate Reductase Trimethoprim Tetrahydrofolic Acid Purines DNA
Pharmacokinetics Given orally fully absorbed from GIT. Distribution:- Widely distributed, in body fluids and tissues, including CSF concentrates in acidic media of prostatic and vaginal fluid. PPB: 65 – 70 % Excretion : in urine within 24 hrs.
Resistance • Reduced cell permeability. • Overproduction of dihydrofolatereductase. • Production of altered reductase with reduced drug binding. Resistance is plasmid encoded.
Clinical Uses • Acute UTI: 100 mg – B.d. • Bacterial Prostatitis (Fluroquinolones are preferred )
CO-TRIMOXAZOLE Combination of trimethoprim with sulfamethoxazole. • Sulfamethoxazole– 400 mg. Ratio 1:5 • Trimethoprim – 80 mg. • One double strength tablet trimethoprim 160 mg • Sulfamethoxazole 800 mg
Advantages of Using Co-Trimoxazole • Bactericidal. (Individual drugs are bacteriostatic) • Wide antibacterial spectrum. • More efficacy. • Less dose of each drug. • Less incidence of toxicity.
PHARMACOKINETICS Can be given orally or I/V
MOA PABA X Dihydropteroate Synthetase Sulfonamides Dihydrofolic Acid (Folate) X Dihydrofolate Reductase Trimethoprim Tetrahydrofolic Acid Purines DNA
Antibacterial spectrum • Gram +ve and gram –ve organisms (resistant to individual drugs) • Chlamydia diphtheriae and N meningitidis. • E. coli, Proteus mirabilis, Proteus marginii, Enterobacterspp, Salmonella, Shigella, Pseudomonas and Serratia are inhibited. • Klebsiella, Brucella, Pasteuralia, Yersinia andNocardia asteroids.
Bacterial Resistance • Plasmid mediated that codes for an altered dihydrofolatereductase.
Pharmacokinetics • Pharmacokinetic profiles of sulfamethoxazole and trimethoprim are closely matched to achieve a constant ratio of 20: 1 in their concentrations in blood and tissues. • Readily enters CSF and sputum. • Excreted through kidneys.
CLINICAL USES 1. Respiratory infections: Pneumocystis jiroveciPneumonia in AIDS patient Hemophilisinfluenzae Streptococcus pneumoniae Moraxella catarrhalis Klebsiellapneumoniae I/V use is for moderate to severe pneumocystis pneumonia, gram-negative bacterial sepsis Caused by multidrug-resistant species.
Acute otitis media in children • Acute maxillary sinusitis in adults.
2. GIT Infections: Shigellosis Systemic Salmonella infection (Typhoid Fever) 3. UTIuncomplicated, complicated and recurrent. 4. Prostatitis 5. Acute Gonococcal Urethritis 6. Non tuberculous mycobacterial infections
Prophylaxis in Neutropenic patients Low dose therapy Emergence of resistant bacteria limit its use. Useful in carriers of Salmonella typhi
Adverse effects • Folate deficient cells • Megaloblasticanemia • Leukopenia • Thrombocytopenia • 75% of untoward effects involve skin • Nausea, vomiting, drug fever, vasculitis, renal damage, CNS disturbances.
Pyrimethamine and sulfonamide • Pyrimethamine + sulfadiazine used for treatment of leishmaniasis and toxoplasmosis. • Pyrimethamine + sulfadoxine used for Falciparum malaria.
Adverse Effects • Hematological • Trimethoprim – Megaloblastic Anemia, Leukopenia, Granulocytopenia • Prevented by simultaneous administrations of folinic acid 6 – 8 mg/D which does not enter bacteria. • Rashes, Fever, Vasculitis
GIT dist. – Nausea, vomiting, Glossitis& stomatitis. • HIV patients with pneumocystis pneumonia shows fever, rashes, leukopenia, diarrhea, elevation of hepatic aminotransferases, hyperkalemia, hypernatremia.