Download
1 / 24
290 likes | 1.02k Views
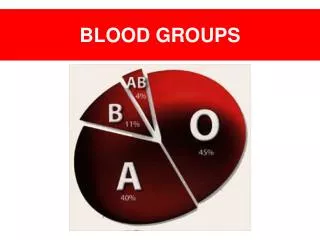
Blood Groups. DIFFERENT BLOOD GROUPS. ABO system. The membrane of RBCs contain antigens of two types (A) and (B) Characters of these antigens are : - inherited according to Mendelian law - appear in fetal life and persist throughout life.

E N D
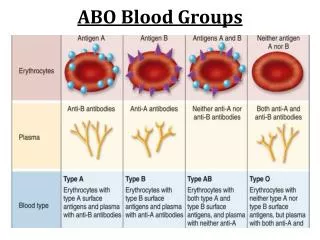
ABO system The membrane of RBCs contain antigens of two types (A) and (B) Characters of these antigens are : - inherited according to Mendelian law - appear in fetal life and persist throughout life. - specific reaction with the corresponding antibodies In the plasma there are antibodies against A and against B and they also are inherited.
According to the types of antigens and antibodies, the blood groups are classified into:
universal recipients universal donors
Importance of blood groups In disputed paternity (good negative test). In the criminal practice. (1) Medicolegal importance: (2) Blood transfusion The recipient’s plasma should not contain antibodies against the donor’s red cells
Incompatible blood transfusion • The donor’s RBCs are agglutinated by recipient plasma • The donor’s serum are diluted by recipient blood so its antibodies are with less or no effect on the recipient RBCs
Rhesus factor (Rh-factor) People are divided according to the presence or absence of Rh- antigen (agglutinogen) on RBCs membrane into: Rh +ve (have D- antigen) = 85% Rh –ve (without D- antigen) =15%.
Rh-antibodies They differ from ABO antibodies in: 1- They are normally absent but induced by blood transfusion of Rh positive blood to Rh-negative patient or in pregnancy.
2- Rh-antibodies are IgG but ABO-antibodies are IgM . - IgM has large molecules and can’t cross placenta - IgG has small molecules and can cross placenta.
Importance of Rh-factor A- Erythroblastosis fetalis Rh +ve male + Rh –ve female Rh +ve fetus Rh +ve fetal RBCs enter the circulation of the mother and sensitize her liver to produce anti- D antibodies (agglutinins).
- Antibodies (IgG) cross the placenta to the Rh +ve 2nd fetus - The 2nd or 3rd fetus is born anaemic, jaundiced or born dead - The 1st baby is also affected if the mother is sensitized by previous transfusion of Rh +ve blood.
Prevention: 1- Rh –ve female should never receive Rh +ve blood 2- Anti-D antibodies are given to the mother during 48 hours after each delivery to neutralize the D-antigen of fetal RBCs transmitted to her prevent formation of liver antibodies Treatment: Gradual replacement of baby’s blood with Rh –ve group O (exchange blood transfusion).
B- Repeated blood transfusion: If Rh –ve person is transfused with Rh +ve blood he will produce antibodies against Rh-factor if this person retransfused with Rh + ve blood agglutination
Determination of blood group: 1- By slide technique
2-By cross matching between recipient and donor blood Group A + Group B = Clumping of RBCs +
Indications: 1) Decrease blood volume (haemorrhage more than 30%). 2) In severe anaemia (Hb is less than 7gm/dl). 3) Restore blood contents as platelets,packed RBCs or clotting factor as in purpura and hemophilia 4) Erythroblastosis fetalis by exchange transfusion.
Precautions 1) Blood is obtained from healthy donors - Age =18-60 year - Weight: more than 55 kgm - Blood pressure within normal range - Hb% is not less than 90% (13gm/dl). - Haematocrit value at least 40%. - Free from infectious diseases as AIDS, viral hepatitis
2) Blood used is stored at 4C not more than 21 days 3) Blood bag must contain, sodium citrate (anti-coagulant), citric acid (reduce pH) and dextrose (nutrient of RBCs) . 4) Blood groups are compatible by double cross matching test 5) The blood is warmed before transfusion to restore the Na-K pump
Complications of blood transfusion A- Incompatibility whichleads to: 1. RBCs are agglutinated in clumps block small blood vessels pain in chest and back 2. Agglutinated RBCs hemolyse and hemoglobin is liberated in plasma and Converted to bilirubin post-transfusion jaundice and precipitated in renal tubules blocking it renal failure .
B- Other complications 1-Transmission of diseases as AIDS & hepatitis B,C. 2- Excessive transfusion heart failure. 3- Hyperkalemia arrhythmia 4- Hypocalcemia tetany 5- Allergic reactions
Changes occur in storedblood 1- Increase K+ ions in plasma (Na-K pump inhibited by cold) . 2- Decrease dextrose and changed to lactic acid. 3- Decrease Platelets number . 4- RBCs swell and become spherical. 5- Decrease clotting factors VII, VIII , IX 6- Decrease 2,3 DPG less O2 supply to the patient hypoxia.