Download
1 / 62
620 likes | 738 Views
Occupational Blood and Bodily Fluid Exposures. Shawn Dowling PGY-1. Despite our best efforts, some occupational exposures will be unavoidable. Objectives. What are blood and bodily fluid exposures? Which diseases are we concerned with? Who gets them? Why???? What can be done?.

E N D
Occupational Blood and Bodily Fluid Exposures Shawn Dowling PGY-1
Despite our best efforts, some occupational exposures will be unavoidable
Objectives • What are blood and bodily fluid exposures? • Which diseases are we concerned with? • Who gets them? • Why???? • What can be done?
Definitions • Health Care Workers: • health-care workers (HCW) are defined as persons whose activities involve contact with patients or with blood or other body fluids from patients in a health-care, laboratory, or public-safety setting • Blood and Bodily Fluid: • Essentially anything that comes out of the patient (other than abusive language), but certain ones (feces, urine, vomitus, saliva) are unlikely to be infectious unless they contain blood
Occupational BBF Exposure • Any time A) comes in contact with B). • Usually classified as percutaneous or mucocutaneous or non-intact skin
Epidemiology • 52% of all HCW report a needlestick injury, 24% had one in the last year • But, estimates are that only 10% of all needlestick injuries are reported
Calgary Health Region #’s Reported blood/bodily fluid exposures in 2003 • FMC - 321 • PLC – 153 • RVH – 134
For the internist….Other possible infections: Blastomycosis Brucellosis Cryptococcosis Diphtheria Cutaneous gonorrhea Herpes Malaria Mycobacteriosis Mycoplasma caviae Rocky Mountain spotted fever Sporotrichosis Staphylococcus aureus Streptococcus pyogenes Syphilis Toxoplasmosis Tuberculosis Transmittable Infections The Big 3: • HIV • Hep B • Hep C
Transmission of HIV/HBV/HCV • Transmitted by semen, vaginal secretions, blood or blood products, breast milk, transplacental transmission or any bodily fluid contaminated with blood • Saliva, feces, urine, vomitus, sputum and tears are not considered infectious unless contaminated with blood • Exceptions: • Vaginal secretions or semen are unlikely to transmit HCV • HBV can be transmitted by saliva
HIV • In general, HIV exposure is low-risk, high consequence • Amount of virus is proportional to risk of infectivity. Therefore viral loads, type of bodily fluid and volume of exposure are important variables to consider
ESTIMATES OF PER-CONTACT RISK OF HIV INFECTION • Occupational Mucocutaneous Exposure 0.09% Important: these numbers are generated via aggregate studies of retrospective and cohort data.
HIV rates in CHR • Prevalence is 0.5%, rate w/ IVDU is 5%
HCW and HIV • From CDC (US data, as of June 2000) • 54 cases reported to have seroconverted after an occupational exposure • 46/54 were percutaneous exposures • 5/54 were mucocutaneous exposures • 2/54 were both • 1/54 unknown • 134 other potential cases (serconverted with no RF, had occupational exposure, but never had blood work done) Surveillance of Health Care Workers with HIV/AIDS, August 2004.
HCW and HIV • Canadian Needle Stick Surveillance Network • Numbers are from 12 sites (8 teaching, 4 community) from April 2000 to March 2002 (ongoing…) • 2,621 occupational exposures to BBF (3.8/100 FTE’s) • Needlesticks: 65.7%, • splashes from patients: 13.7%, • cuts with sharp objects: 8.6%, • sticks other than needles: 7.2%, • Others: scratches 1.9%, direct contacts with patients 1.8% (i.e. touching patients directly) and bites with broken skin 1.2% • Prevalence of HCV = 7.6%, HIV = 2.6% and HBV = 1.8% amongst source patients • As a result the rate of exposure to infected BBF was 0.3%
Hep B • Although percutaneous is the most efficient route of transmission, these likely only account for a minority, • In several studies, HCW could not recall an overt percutaneous injury, • And since HBV can survive in at room temp for a week, transmission is thought to primarily arise from contact with cuts, abrasions or mucosal surfaces 95% 5%
Best transmitted via percutaneous exposure Minimal risk w/mucous membranes or contact with blood Crappy dz (since no PEP, but fortunately, but risk of transmission is low) Hep C 15% 85%
Case • 78 yr female, security guard at the PLC, is waiting to be seen in the MT area. An hour ago she was involved in an alteration with an agitated patient. Both were bloodied in the battle and the security guard is concerned about getting HIV. • When you go to see her, she’s still covered in blood. What do you do?
If you do get poked/exposed • Remove the contaminated clothes – undergarments excepted • Allow immediate bleeding of the wound • Wash the injured area well with soap and water, and apply an antiseptic • If the eyes, nose, or mouth are involved, flush them well with large amounts of water
Prevention • Universal Precautions: Treat everyone as if they may have HIV/HBV/HCV • In 1985, 94% of all AIDS patients had a major RF • In 1996, 20% of all patients had been infected through heterosexual contact or had no known RF • Protect your self • Handwashing • Gloves • Masks • Eye protection • Face shields • Gowns/aprons • Safety Measures • Don’t recap needles, avoid being a surgical resident, safety intravenous catheters, dispose sharps
Report all cases • Call OH & S Nurse (234-7799) • Available 24 hrs/day • Provides patient with appropriate f/u • Will do Risk Assessment • Allows for surveillance/monitoring
Southern Alberta Clinic Guidelines • Is the source known HIV+? • Yes: proceed to step 2 of protocol • No: • Test source (with consent) using rapid point-of-care HIV test available through CLS at any Emergency Room or 8th and 8th health centre • If negative, and no risk of “window period”, reassure patient • If source unknown or refuses testing and has risks for or symptoms of HIV, proceed to step 2 of protocol • Consider source testing for HBV, HCV – most guidelines suggest testing for this
Rapid HIV Testing • Sensitivity and Specificity both 99.9% • Done in the on-site rapid response labs • Current turn around time 1 hr 24 min • Confirmed by Western Blot at Prov Lab • Consider giving dose of PEP before results arrive (based on your pre-test probability) • Cost: considerable, but should not play a factor
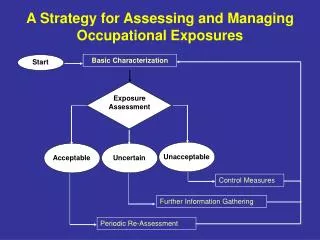
Timing and Type of Exposure: • Assess fluid type, volume, viral titre, mode of exposure. • Assess exact timing of exposure • If exposure is not considered infectious for HIV/HBV/HCV (i.e. vomit, feces, etc. without blood – see slide #10) – reassure and arrange f/u if patient desires • If exposure considered potentially infections go to 3.
Decision: • Make a decision for or against PEP based on risk assessment (these are debatable) • HIV + = start PEP • HIV – and no risk of source pt being in “Window period” = don’t start PEP • Unknown (source not tested or refuses testing) = this is where you earn your money • HEP B – see slide 54-55 on HBIG and Hep B vaccine
Unknown HIV status: What to do? • Determine: • Type of exposure (percutaneous v mucous membrane) • Source risk/setting: needlestick risk different at 8th and 8th clinic compared to Geriatric assessment unit • In these scenarios, need to have an in-depth conversation with patient to determine management/risk tolerance but…fortunately, there are some consensus guidelines
High risk IVDU High risk sexual behaviour (MSM, sex w/IVDU, multiple sexual partners (3 or more sexual partners/yr w/I past 5 yrs), prostitution Blood transfusion prior to 1985 Sex w/HIV + person Clinical suspicion of HIV infections by physicians Prior HIV test HIV as part of a Ddx Unexplained opportunistic infections (i.e. PCP, toxo, crypto, histo, TB, MAC) Low Risk HIV - Serology unknown but answers no to all high risk questions Unknown Source is not assessed Risk Assessment-In general, Should be done by OH&S
Drug Selection • Best to start within 1-2 hrs, consider dose before Rapid HIV test returns depending on risk of source patient • Basic Regimen: • If Low risk exposure (unknown source or mucocutaneous exposure) • Combivir: (AZT 300mg + 3TC 150mg) bid • Expanded Regimen: • For most percutaneous to known HIV + • Basic Regimen + Nelfinavir 1250mg bid • Other: • consider other drugs if source patient is already on antiretrovirals or if source patient is known to have resistant HIV
Duration of Prophylaxis: • Start ASAP and continue for 4 weeks • Discuss adverse reactions w/patient:
Access and Cost: • Starter kits contain 72 hours of drugs • Free for occupational exposure and non-voluntary or violent (assault) exposures • Non-occupational voluntary exposures (needles or sex): PEP is available, but cost not absorbed by CHR • In Calgary, starter kits are available in all hospital ED’s, and at the 8th & 8th 24-hour walk-in medical clinic. All antiretroviral drugs are stored in the Pharmacy at Foothills Medical Centre. • Cost: approx $1000 for 4 wks of combivir
A Few Words about PEP • Theoretically, initiation of antiretroviral PEP soon after exposure might prevent or inhibit systemic infection by limiting the proliferation of virus in the initial target cells or lymph nodes – most studies are done in animals or in vertical HIV transmission
Case-Control Study • Primary outcome: • Risk Factors for acquiring HIV after a HCW has a percutaneous exposure • 712 patients • 679 retrospective controls (no seroconversion after exposure @ 6 months) • 33 prospective Cases (seroconversion after exposure)
Factors not Associated w/HIV transmission • Large bore needles • Use of gloves • Hollow bore vs. suture needles
Study quotes a 80% (CI 43-94%) reduction rate of HIV transmission with use of AZT • ARR = 0.24%, NNT= 417 • An nationwide RCT was attempted, but only able to recruit 84 patients over a year --- I wonder why?
Human Studies • Generally poor • NEJM is the best study to look at AZT use and seroconversion in Human occupational exposures, but it was small and used different cohorts, retro/prospective, inconsistent data availability, and relied on recall
Human Studies • Lots of studies looking at vertical HIV transmission • Quote reduction rates from 37-67% (depending on when started) • Problem of the benefit is secondary to decreasing mom’s viral load and therefore decreasing infectivity, therefore numbers are not applicable to occupational exposures
Animal Studies • Challenges • identifying an animal model that is comparable to humans • In early studies, differences in controlled variables (e.g., choice of viral strain [based on the animal model used], inoculum size, route of inoculation, time of prophylaxis initiation, and drug regimen) made results very heterogeneous
Animal Studies • Studies among animal models have demonstrated that larger viral inocula decrease prophylactic efficacy • Delaying initiation, shortening the duration, or decreasing the antiretroviral dose of PEP decreased prophylactic efficacy
PEP Side Effects/Adverse Events • Divided into Major and Minor • Minor: experienced by 50 - 80% • nausea (57%) • Vomiting & Diarrhea (14% & 16%) • Headache (18%) • Fatigue or Malaise (38%) • Mean time to onset of symptoms 3 or 4 days for all of the above
Major: defined as life threatening, permanent or requiring hospitalization • Serious side effects, including nephrolithiasis, hepatitis, and pancytopenia have been reported with the use of combination drugs for PEP • One case of NVP (NNRTI)-associated fulminant liver failure requiring liver transplantation
Compliance • 33% stopped the PEP prematurely • s/e and discontinuing PEP are seen more frequently with triple-therapy (indinavir is particularly nasty) • If pt started on triple therapy and complains of a/e and wants to d/c, stop 3rd Rx first as this is most likely causing the worse Sx • Educating pts about s/e, a/e has been shown to increase compliance
PEP Failure • Failure of PEP to prevent HIV infection in HCW has been reported in at least 21 instances • In 16 of the cases, ZDV was used alone as a single agent (currently not recommended) • In 2 cases, ZDV and didanosine (ddI) were used in combination • In three cases, 3 drugs were used for PEP • 13 of the source persons were known to have been treated with antiretroviral therapy before the exposure. Antiretroviral resistance testing of the virus from the source person was performed in seven instances, and in four, the HIV infection transmitted was found to have decreased sensitivity to ZDV and/or other drugs used for PEP. • Other factors come in to play: compliance, viral load, inoculum, etc