Download
1 / 35
460 likes | 919 Views
EQ-5D, HUI and SF-36 . Of the shelf instruments…. Direct valuation. …or use validated questionnaires. MOBILITY I have no problems in walking about I have some problems in walking about I am confined to bed SELF-CARE I have no problems with self-care

E N D
EQ-5D, HUI and SF-36 Of the shelf instruments….
…or use validated questionnaires MOBILITY • I have no problems in walking about • I have some problems in walking about • I am confined to bed SELF-CARE • I have no problems with self-care • I have some problems washing or dressing myself • I am unable to wash or dress myself USUAL ACTIVITIES (e.g. work, study, housework family or leisure activities) • I have no problems with performing my usual activities • I have some problems with performing my usual activities • I am unable to perform my usual activities PAIN/DISCOMFORT • I have no pain or discomfort • I have moderate pain or discomfort • I have extreme pain or discomfort ANXIETY/DEPRESSION • I am not anxious or depressed • I am moderately anxious or depressed • I am extremely anxious or depressed
The Rosser & Kind index One of the oldest valuation 1978: Magnitude estimation Magnitude estimation PTO / VAS N = 70 Doctors, nurses, patients and general public 1982: Transformation to “utilities” On a 0.00 to 1.00 scale Could be used for QALYs
1985: High impact article • Survey at the celebration of 25 years of health economics in the UK (HESG): chosen most influential article on health economics
Criticism on the Matrix Sensitivity only 30 health states The unclear meaning of “distress” The involvement of medical personnel No clear way how to classify the patients into the matrix Only British values The compression of states in the high values
New initiatives • Higher sensitivity (more then 30 states) • More and better defined dimensions • Other valuation techniques • Standard Gamble, Time Trade-Off, Visual Analogue Scale • Values of the general public • A questionnaire… • to allow patients to ‘self classify’ themselves • An international standard • to allow international comparisons • That is at that time “Europe”
No longer value all states • Impossible to value all health states • If one uses more than 30 health states • Estimated the value of the other health states with statistical techniques • Statistically inferred strategies • Regression techniques • EuroQol, Quality of Well-Being Scale (QWB) • Explicitly decomposed methods • Multi Attribute Utility Theory (MAUT) • Health Utility Index (HUI)
Statistically inferred strategies • Value a sample of states empirically • Extrapolation • Statistical methods, like linear regression • 11111 = 1.00 • 11113 = .70 • 11112 = ?
Statistically inferred strategies • EuroQol • EQ-5D: 5 dimensions of health • 245 health states • Quality of Well-Being scale (QWB) • 4 dimensions of health • 2200 health states plus 22 additional symptoms • SF-36 • SF-6D: 6 dimensions of health • 18.000 health states
Explicitly Decomposed Methods • Value dimensions separately • Between the dimensions • What is the relative value of: • Mobility…... 20% • Mood…….. 15% • Self care.… 24%. • Value the levels • Within the dimensions • What is the relative value of • Some problems with walking…… 80% • Much problems with walking…... 50% • Unable to walk…………………….10% • 21111 = 1 - (0.20 x (1.00 - 0.80)) = 0.96
Explicitly Decomposed Methods • Combine values of dimensions and levels with specific assumptions • Multi Attribute Utility Theory (MAUT) • Mutual utility independence • Structural independence
Explicitly Decomposed Methods • Health Utilities Index (Mark 2 & 3) • Torrance at McMaster • 8 dimensions • Mark 2: 24.000 health states • Mark 3: 972.000 health states • The 15-D • Sintonen H. • 15 dimensions • 3,052,000,000 health states (3 billion)
Exercise • EuroQol EQ-5D (3 level) • SF-6D
More health states, higher sensitivity ? (1) • EuroQol criticised for low sensitivity • Low number of dimensions • Development of EQ-5D plus cognitive dimension • Low number of levels (3) • Gab between best and in-between level • Now development of 5 Level • EQ-5D-5L • No consensus in EuroQoL that more levels is always better…
More health states, higher sensitivity ? (2) • Little published evidence • Sensitivity EQ-5D < SF-36 • Compared as profile, not as utility measure • Sensitivity EQ-5D HUI • Sensitivity the number of health states • How well maps the classification system the illness? • How valid is the modelling? • How valid is the valuation?
More health states, more assumptions • General public values at the most 50 states • The ratios empirical (50) versus extrapolated • Rosser & Kind 1:1 • EuroQol EQ-5D-3L 1:5 • QWB 1:44 • EQ-5D-5L 1:63 • SF-36 1:180 • HUI (Mark III) 1:19,400 • 15D 1:610,000,000 • What is the critical ratio for a valid validation?
SF-36 as utility instrument • Transformed into SF6D • SG • N = 610 • Inconsistencies in model • 18.000 health states • regression technique stressed to the edge • Floor effect in SF6D
Collapsing levels SF-6D • Many levels are taken together • If PF=2 decrement: - 0.056 • If PF=3 decrement: - 0.056 • If RL=2 decrement: - 0.073 • If RL=3 * decrement: - 0.073 • If RL=4 * decrement: - 0.073
SF-6D loses a lot of levels • Levels in system and actual levels • PF 6 5 • RL 4 2 • SF 5 5 • PN 6 5 • MH 5 4 • VI 5 3 • Levels in system: 18.000 • 6x4x5x6x5x5 • Actual levels: 480 • 5x2x5x5x4x3
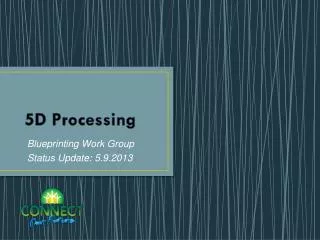
Conflicting evidence sensitivity SF-36 Liver transplantation, Longworth et al., 2001
EQ-5D-3L • Strong punts • Very sensitive in the low • Measures subjective burden (inside the skin) • Low administrative burden • Many translations • Cheap • Most used QALY questionnaire • Most international validations • Weak points • Only there levels per dimensions • Insensitive in the high regions
EQ-5D-5L • Strong punts • Very sensitive in the low • Measures subjective burden (inside the skin) • Low administrative burden • Many translations • Cheap • Weak points • No scorings algorithm yet • Might still not be as sensitive in the high regions
HUI • Strong punts • Sensitive • Measures objective burden (outside the skin) • Well developed proxy versions • Well developed child versions • Weak points • Expensive
SF-6D • Strong punts • Probably sensitive in the high regions • Often already include in trials (SF-36) • Cheap …. • Many translations • Weak points • Insensitive in the low regions • Only one validation study • Changed Standard Gamble • Upwards shift of values
No scoring algorithm EQ-5D-Y
Conclusions More states better sensitivity The three leading questionnaires have different strong and weak points