Download
1 / 18
230 likes | 632 Views
DISORDERS OF NERVOUS SYSTEM. Dr. Saleem Shaikh. Introduction. Divisions of the nervous system: Central Nervous System Brain and spinal cord Peripheral Nervous System Peripheral nerves Autonomic Nervous System Symphathetic nervous system Parasympathetic nervous system. Common disorders.

E N D
DISORDERS OF NERVOUS SYSTEM Dr. SaleemShaikh
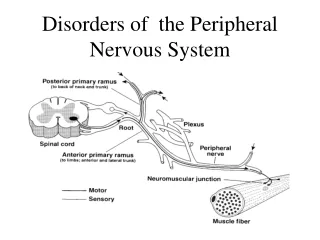
Introduction • Divisions of the nervous system: • Central Nervous System • Brain and spinal cord • Peripheral Nervous System • Peripheral nerves Autonomic Nervous System • Symphathetic nervous system • Parasympathetic nervous system
Common disorders • Headaches (Migraine) • Alzheimer’s disease • Cerebrovascular accident – stroke • Epilepsy • Meningitis • Poliomyelitis • Neuralgias • Tumors
Headaches • Any pain occurring in the head • Acute or chronic • Numerous etiologies • Very common condition • May be a symptom of other diseases • Infections, neoplasms, inflammatory diseases, etc • Due to irritation, inflammation of any pain-sensitive structure • Brain itself is not a source of headache
Migraine Headache • Migraine is a term applied to certain headaches with a vascular quality, characterized by varying degrees of recurrent vascular headache, photophobia, sleep disruption, and depression. • mechanisms of migraine are not completely understood. • Migraine usually begins during the second decade of life and is especially common in professional persons. • The frequency of attacks is extremely variable. They may occur at frequent intervals over a period of years or on only a few occasions during the lifetime of the patient.
A prodromal stage (preheadache phenomenon) is noted by some patients, consisting of lethargy and dejection several hours before the headache. Visual phenomena such as scintillations, hallucinations are often described • The headache phase consists in severe pain in the temporal, frontal and retro-orbital areas. • The pain is usually unilateral • The pain is usually described as a deep, aching, throbbing type. • Anorexia and vomiting may occur, as well as a variety of visual disturbances. Prolonged and painful contraction of head and neck muscles is found in some patients. • Treatment: The treatment of migraine includes a wide variety of drugs ranging from acetylsalicylic acid and codeine to ergotamine, methysergide and norepinephrine.
Neuralgia • Neuralgia is pain in one or more nerves that occurs without stimulation of pain receptor (nociceptor) cells. • Examples: • Trigeminal neuralgia • Sphenopalatine neuralgia
Trigeminal neuralgia • Trigeminal neuralgia (“tic douloureux”) follows the anatomical distribution of the fifth cranial nerve. It mainly affects the second and third divisions of the trigeminal nerve. • Most cases are idiopathic, but compression of the trigeminal roots by tumors or vascular anomalies may cause similar pain • . • The pain itself is of a searing, stabbing, or lancinating type which many times is initiated when the patient touches a “trigger zone” on the face. • Each attack of excruciating pain persists for only a few seconds to several minutes and characteristically disappears as promptly as it arises. • the pain may be so severe that the patient lives in constant fear of an attack, and many sufferers have attempted suicide to put an end to their torment.
The “trigger zones,” which precipitate an attack when touched, are common on the vermilion border of the lips, the alae of the nose, the cheeks, and around the eyes. Usually any given patient manifests only a single trigger zone. • Treatment: • One of the earliest forms of treatment was peripheral neurectomy, • Injection of alcohol either into a peripheral nerve area or centrally into the gasserian ganglion. • Carbamazepine is the drug of choice in recent times • microsurgical decompression of the trigeminal root
SphenopalatineNeuralgia • Sphenopalatine ganglion neuralgia, or periodic migrainous neuralgia, is characterized by unilateral paroxysms of intense pain in the region of the eyes, the maxilla, the ear and mastoid, base of the nose, and beneath the zygoma. • These paroxysms of pain have a rapid onset, persist for about 15 minutes to several hours, and then disappear as rapidly as they began. There is no “trigger zone.” • Interestingly, in some patients the onset of the paroxysm occurs at exactly the same time of day and, for this reason, the disease has been referred to as “alarm clock” headache.
Auriculotemporal Syndrome • Frey’s Syndrome • which arises as a result of damage to the auriculotemporal nerve and subsequent reinnervation of sweat glands by parasympathetic salivary fibers. • The patient typically exhibits flushing and sweating of the temporal area during eating. • similar condition known as “crocodile tears” • The syndrome is a possible complication of parotitis, parotid abscess, parotid tumor and ramusresection
Bell’s Palsy • Bell’s palsy is paralysis of the facial musculature, usually unilaterally. • The muscular paralysis manifests itself by the drooping of the corner of the mouth, from which saliva may run, the watering of the eye, and the inability to close or wink the eye. • . When the patient smiles, the corner of the mouth does not rise. The skin of the forehead does not wrinkle. The patient can not raise his/her eyebrow. • The patient has a typical masklike or expressionless appearance. Speech and eating usually become difficult. • Sometimes the taste sensation on the anterior portion of the tongue is lost or altered. • Usually idiopathic but facial nerve paralysis may be seen as a complication of inferior alveolar nerve block. • Melkersson-Rosenthal syndrome
Alzheimer’s disease • Alzheimer’s disease is a brain disease that slowly destroys memory and thinking skills and, eventually, the ability to carry out the simplest tasks. It begins slowly and gets worse over time. Currently, it has no cure. • Dementia is a loss of thinking, remembering, and reasoning skills that interferes with a person’s daily life and activities. • Alzheimer’s disease is the most common cause of dementia
Disorders that cause paralysis • Hemiplegia • Loss of muscle control & sensation on one side of the body (Lefror Right) • Paraplegia • Loss of muscle control & sensation on the lower part of the trunk and lower extremities • Quadriplegia • Paralysis of all four extremities
Cerebrovascular Accident (CVA) • Focal neurological impairment due to lack of blood supply to an area of the brain lasting more than 24 hours • Clinical condition is called stroke • 2 types of stroke: • Ischemic: embolic or thrombotic, 75% CVA’s • Hemorrhagic: 25% CVA’s • Risk factors: same as for cardiovascular disease, smoking, HTN, hyperlipidemia, diabetes, etc. TIA’s, oral contraceptives • Clinical features: hemiplegia or hemiparesis, dysphagia, speech impairment, diplopia & loss of visual fields, lack of coordination, confusion, sensory impairment