Download
1 / 83
840 likes | 869 Views
Dept. of General and Transplant Surgery. Diseases of the pancreas. Jakub Szmytkowski. Anatomy - location. Retroperitoneal (except part of the tail) in the epigastrium and left infracostal region Approximate dimensions: L 15 cm, W 3-4 cm, T 1-2 cm; weight 60-100 g. Anatomy - parts. head

E N D
Dept. of General and Transplant Surgery Diseases of the pancreas Jakub Szmytkowski
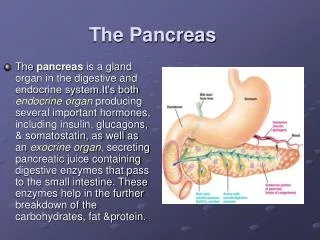
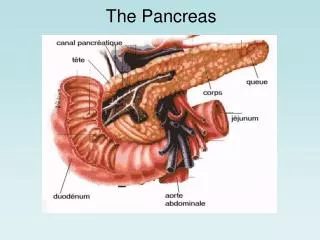
Anatomy - location • Retroperitoneal (except part of the tail) in the epigastrium and left infracostal region • Approximate dimensions: L 15 cm, W 3-4 cm, T 1-2 cm; weight 60-100 g
Anatomy - parts • head • Isthmus (notch) • uncinate process • body • tail
Pancreatic ducts • Thepancreaticduct, orduct of Wirsung (also, the major pancreaticduct)a ductjoiningthepancreas to thecommon bile duct to supplypancreaticjuiceswhichaidindigestionprovided by the "exocrinepancreas". Thepancreaticductjoinsthecommon bile ductjustprior to theampulla of Vater, afterwhichbothductsperforatethemedialside of thesecondportion of theduodenumatthe major duodenalpapilla.
Pancreatic ducts • Accessory pancreatic duct (duct of Santorini) connects straight to the duodenum at the minor duodenal papilla • In some cases, the main pancreatic duct is smaller than the accessory pancreatic duct and the two may not be connected. In such people, the accessory duct carries most of the pancreatic juice.
Anatomical relations • anterior: transverse colon (head) pylorus (body) • posterior: VCI, CBD, aorta, superior mesenteric a., renal veins • left: splenic hilus, splenic flexure • right: duodenum • superior: celiac trunk, splenic a.
Surgical diseases of the pancreas • Acute pancreatitis • Chronic pancreatitis • Cysts • Tumors
Goals of pancreatic surgery • Completion of diagnosis • Treatment of pancreatitis • Treatment of infection and complications • Paincontrol • Malignanttumors • curative • palliative • Management of endocrinedisorders
Acute pancreatitis • Acutepancreatitisis a complexdisorder of theexocrine part of thepancreas. Itsexactpatomechanismhas not beenfullyexplained, but can be described as acuteinjury to theacinarcellswith a local and generalizedinflammatoryresponse. • Overallmortality6.0-20.5% • Necrotizing – hemorrhagic (5 – 15%) 50+% • Morbidity (Poland) 240 / 100 000 / year • No specifictherapy
Types • interstitial edematous pancreatitis • sterile necrotizing pancreatitis • infected pancreatic necrosis/abscess • hemorrhagic pancreatitis
Frequent causes • gallstones • alcohol • idiopathic • hyperlipidemia • hypercalcemia • drugs and toxins ( steroids, immunosuppressants: Azathioprine, Thiazide, Valproic acid, Tetracycline, and Trimethoprim-sulfamethoxazole ) • endoscopic retrograde cholangiopancreatography • trauma • surgery 80%
Less frequent causes • Malignancies of theampulla of Vater • Pancreatic carcinoma • Diverticulum of theduodenum • Vasculitis
Even less frequent causes • infection: viral (Coxsackie, mumps , HIV), parasites • Autoimmunedisorders: lupus, Sjögren’ssyndrome • alpha1-antitripsin deficiency • Anorexia • Repeatedmarathonrunning • Scorpionvenom • Pancreasdivisum
Physiology • Thepancreassecretes500-800 ml/day of transparent, anodorous, isoosmoticjuicewith a high pH, containingbicarbonates and digestiveenzymes • Stimulants: secretin, duodenalpH <4.0 • Cholinergicstimulation – vagusnerve
Physiology • The proportions of different enzymes differ; various nutrients stimulate the secretion of various enzymes • Cholecystokinin (CCK) i s the primary regulator • Secondary mediators include Ca++ and diacylglycerol
Pancreatic enzymes • Amylase Active • Proteases ( trypsin) Inactive • LipasesInactive • Inhibitors: • Alpha 1-antitrypsin • Beta2-macroglobulin • Pancreatic secretory trypsin inhibitor (PSTI)
Pathology • overpressureinWirsung’sduct • abnormalinhibition of secretion of zymogens and inappropriateactivation of pancreaticzymogensinsidethepancreas, most notablytrypsinogen • during an acutepancreatitisepisodethereiscolocalization of lysosomalenzymes, specificallycathepsin, withtrypsinogen. Cathepsinactivatestrypsinogen to trypsinleading to furtheractivation of othermolecules of trypsinogen and immediate pancreaticcelldeathaccording to eitherthenecrosisorapoptosismechanism(or a mix betweenthetwo)
Pathology • an extensive inflammatory response due to pancreatic cells synthesizing and secreting inflammatory mediators: primarily TNF-alpha and IL-1 • inflammatory response leads to the secondary manifestations of pancreatitis: hypovolemia from capillary permeability, acute respiratory distress syndrome, disseminated intravascular coagulations, renal failure, cardiovascular failure, and gastrointestinal hemorrhage
Signs and symptoms • SEVERE abdominalpain – usually (95-100%) first symptom, oftenradiates to the back • Nausea,vomitingwithout relief ( 80%) • Fever (onsetcrucial for correct management: 1st week – SIRS; 2 weeks and later – necrosisinfection) • Epigastrictenderness • Peristalticsoundsweakorabsent (paralyticileus)
Signs and symptoms • Tender epigastric mass – parapancreaticinfiltration • Shock • Pancreaticencephalopathy • Tachycardia (often) • Hypotonia (due to hypovolemia) • Jaundice – (20-30%)
Loeffler’s sign – facial erythema Clairmont’s sign – left pleural effusion Körte's sign (pain or resistance in the zone where the head of pancreas is located (in epigastrium, 6–7 cm above the umbilicus)) Kamenchik's sign (pain with pressure under the xiphoid process) Mayo-Robson's sign (pain while pressing at the top of the angle lateral to the Erector spinae muscles and below the left 12th rib (left costovertebral angle (CVA)) Rare sypmtoms
Grey Turner's sign • bruising of the flanks, appearing as a blue discoloration • a sign of retroperitoneal hemorrhage • Also seen in: • Blunt abdominal trauma • Ruptured abdominal aortic aneurysm • Ruptured / hemorrhagic ectopic pregnancy
superficial edema and bruising in the subcutaneous fatty tissue around the umbilicus Cullen's sign
bruising along inguinal ligament Fox’s sign
Symptoms - summary Abdominalpain 85-100% Nausea and vomiting 55-90% Anorexia 80% Tachycardia 65-80% Fever 12-80% Bowelobstruction 50-80% Tender abdominal mass 90-99% All of themnon -specific Baron TH, Morgan DE. Acute Necrotizing Pancreatitis, NEJM, 1999
Lab results indicative of AP • Elevated serum amylase and lipaselevels no role inassessingdiseaseseverity. • Serum lipaserises 4 to 8 hoursfromtheonset of symptoms and normalizeswithin 7 to 14 daysaftertreatment • Serum amylasemay be normal(in 10% of cases) for cases of acuteorchronicpancreatitis (depletedacinarcell mass) and hypertriglyceridemia. • Reasons for falsepositiveelevated serum amylaseincludesalivaryglanddisease (elevatedsalivaryamylase), bowelobstruction, infarction, cholecystitis, and a perforatedulcer. • Ifthelipaselevelisabout 2.5 to 3 timesthat of amylase, itis an indication of pancreatitisdue to alcohol • Decreased serum calcium • Glycosuria • Increased CRP
Acutepancreatitis: US imaging • Abdominal US usuallyperformed pancreasofteninvisible (intestinalgasses, obesity) • US inacutepancreatitis: pancreasenlarged, boundaries not clearlydefined (inflammatoryinfiltration), heterogenousechogenicity • US important for ID of causativefactor (gallstones) • Monitoring of complications (abcess, cyst, necrosis)
Computedtomography • „Gold standard” in AP imaging; enablesassessment of severity and necroticchanges (Balthasar score A-E) • Helpsassessseverity (CTSI index) • Recommendedafter 72 h fromonset of symptoms, • In criticalpatients – immediate CT • Furtherscansafter 7-10 daysor upon significantchanges of patient’scondition
Necrosisscore CTSI score = Balthasar + necrosisscore
Otherimagingmodalities • ChestX-ray • Interstitalatelectasis, pleuraleffusion, ARDS • AbdominalX-ray • Fluid levels, boweldistension (signs of paralyticileus) • MR • indication for imaging of patients with an allergy to CT's contrast material
Course of the disease • Edematous AP (60-70%) of thepatients – treatment of symptoms, no complications, mortality < 1% • Severe AP (30-40% )– mortalitybetween 10% (sterilenecrosis) and 25% (infectednecrosis); if organ – specificcomplicationsarise, themortalityratesincrease to 20% and 50-80% , respectively. • insevere AP therearetwoperiods of increasedmortality: • early (~60% deaths) – first 7-14 days: early MOF, severe ARDS due to SIRS • late (~40% deaths) – 3-4 weeksfromonsetinfection of necrotictissues, abscessformation sepsis septicshock MOF
AP severityscores • Ransoncriteria for non – gallstone AP • At admission: • Age in years > 55 years • White blood cell count > 16000 cells/mm3 • Blood glucose > 10 mmol/L (> 200 mg/dL) • Serum AST > 250 IU/L • Serum LDH > 350 IU/L
After 48 hrs Serum calcium < 2.0 mmol/L (< 8.0 mg/dL) Hematocritfall > 10% Oxygen (hypoxemia PO2 < 60 mmHg) BUN increased by 1.8 ormoremmol/L (5 ormore mg/dL) after IV fluid hydration Basedeficit (negativebaseexcess) > 4 mEq/L Sequestration of fluids > 6 L
Ranson for gallstone AP At admission: Age in years > 70 years White blood cell count > 18000 cells/mm3 Blood glucose > 12.2 mmol/L (> 220 mg/dL) Serum AST > 250 IU/L Serum LDH > 400 IU/L
After 48 hrs Calcium (serum calcium < 2.0 mmol/L (< 8.0 mg/dL) Hematocritfall > 10% Oxygen (hypoxemia PO2 < 60 mmHg) BUN increased by 1.8 ormoremmol/L (5 ormore mg/dL) after IV fluid hydration Basedeficit (negativebaseexcess) > 5 mEq/L Sequestration of fluids > 4 L
Ranson - interpretation If the score ≥ 3, severe pancreatitis likely. If the score < 3, severe pancreatitis is unlikely Or: Score 0 to 2 : 2% mortality Score 3 to 4 : 15% mortality Score 5 to 6 : 40% mortality Score 7 to 8 : 100% mortality
Conservativetreatment • Anti –shock treatment • Pain control • Nil-by-mouth regime • Nasogastric tube placement • Total parenteral nutrition • Stress ulcer prevention • Wide - spectrum antimicrobial • Fluid replacement therapy
Endoscopicretrogradecholangiopancreatography(ERCP) • combines the use of endoscopy and fluoroscopyto diagnose and treat certain problems of the biliaryor pancreatic ductal systems • plastic catheter inserted through the ampulla, and radiocontrast is injected into the bile ducts and/or pancreatic duct. Fluoroscopy is used to look for blockages, or other lesions such as stones
ERCP • opening of the ampulla can be enlarged (sphincterotomy) with an electrified wire (sphincterotome) and access into the bile duct obtained • trawling of the common bile duct with a basket or balloon to remove gallstones and the insertion of a plastic stent to assist the drainage of bile • directelectrohydrauliclithotripsy
Indications for surgery • Diagnosis uncertain( peritoneal signs) • Symptoms of necrosis infection or abscess • Complications: bowel necrosis, perforation, hemorrhage
Timing of surgery • Almost never before 10th day after onset – unless fulminating necrosis occurs • surgery 0 – 7th day - mortality 38% • surgery 8 – 14th day - mortality 28% • surgery >21 day - mortality. 15% • Complete necrosis facilitates removal
The role of surgery in severe AP • Necrectomy, lavage / drainage of the bursa omentalis • laparostomy • abscessdrainage • debridement of theretroperitonealspace