Download
1 / 46
470 likes | 505 Views
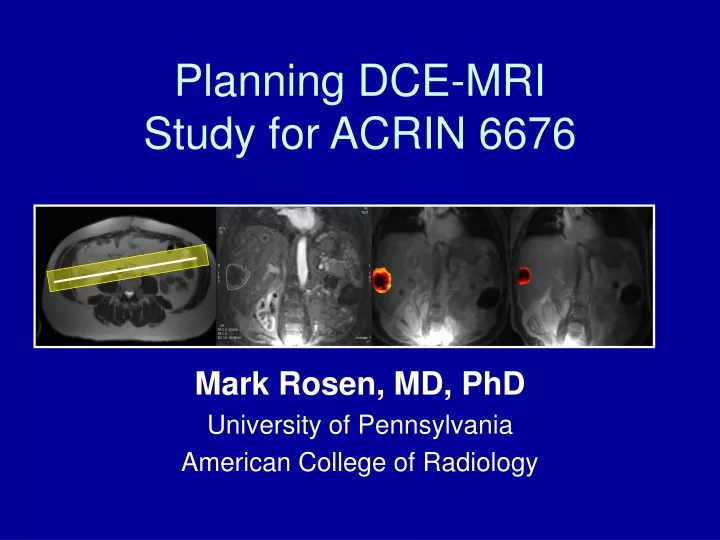
Planning DCE-MRI Study for ACRIN 6676. Mark Rosen, MD, PhD University of Pennsylvania American College of Radiology. Site Qualification. All DCE-MR sites must complete Form QC and receive approval of phantom imaging. Contact the ACRIN MR Core Lab at 215-940-8880 for details.

E N D
Planning DCE-MRIStudy for ACRIN 6676 Mark Rosen, MD, PhD University of Pennsylvania American College of Radiology
Site Qualification • All DCE-MR sites must complete Form QC and receive approval of phantom imaging • Contact the ACRIN MR Core Lab at 215-940-8880 for details
Patient Entry Criteria • Metastatic or locally advanced ccRCC • Must be enrolled in treatment trial E2804 • Must have at least one qualifying lesion • based on size, morphology and location
Definition of Qualifying Lesion • Lesion must be in anatomic region which can be covered using a torso array coil • Lower neck through thighs • Includes upper arms • Excludes skull, upper neck, distal extremities • > 2 cm in “fixed” sites: • spine, pelvis, extremities • retroperitoneum, posterior chest wall • > 3 cm in “mobile” sites: • Lungs, liver, kidneys, anterior chest wall
Identification of Target Lesion • Review pre-enrollment imaging results • Select target lesion for DCE-MRI • Meets size criteria • Not largely necrotic • Away from regions of pulsatility • (such as heart, hila, left lateral segment of liver)
Optimizing Choice of Target • If more than one candidate lesion, choose lesion in area with least degree of anatomic motion • Pelvis/extremities/spine/post. chest wall (preferred) • Retroperitoneal nodes (next best) • Upper lungs (next best) • Liver/kidney (next best) • Lower lungs, ant. chest wall (least preferred)
DCE-MRI Patient Set-up • IV placement prior to entry onto scanner* • Position patient supine • Torso coil centered to lesion location • Arm position above head • If arms cannot be positioned above head… • If lesion is posterior, then position arms across chest • keep IV site patent and flowing • If lesion is anterior, then position arms at sides • Landmark as close as possible to area of target lesion • IV KVO with normal saline during DCE-MRI study *Central venous access can be used if this is the only available venous access, per institutional policies and in discussion with referring oncologist. If central access is not rated for power injection, hand injection at approximately 1cc/sec can be used.
Sequence List • 3 Plane Loc • Axial T1 • Axial T2 SSFSE T1 Maps: • 30 Flip (Auto Pre-scan) • 15 Flip (NO PRE-SCAN) • 5 Flip (NO PRE-SCAN) Dynamic: • 30 Flip (Inject .1mmol/kg @1cc/sec, 20cc flush) (NO PRE-SCAN) • Run ~6 minutes with 20-30 seconds of baseline • #phases depends on temporal resolution Delayed Coronal in the SAME OBLIQUE PLANE with FatSat Delayed Axialof entire anatomic region (i.e. lungs, pelvis, etc.)
Preliminary Sequences • Localizer • Axial T1 • Recommended: Dual-echo FSPGR/FLASH • Axial T2 • Recommended: SS-FSE/HASTE, TE=90, no fatsat Notes for axial sequences: • Always during end expiration • May perform with multiple breath holds if necessary • Slices thickness 5-8 mm • Cover entire anatomic region • e.g. lungs, liver/abdomen, pelvis
Optimizing Choice of Target • Identify target lesion from axial scans • If more than one potential lesion… • Choose lesion with following characteristics • Non-necrotic, non hemorrhagic • Well-marginated • 3-6 cm (better than much larger lesions)
Oblique slab placement • Parameters for oblique slab (FOV, slice thickness, # of slices, matrix), are determined from site phantom imaging and Form QC. • From axial image (T1 or T2) identify middle slice through lesion • Prescribe oblique 3D slab to bisect both lesion and aorta • Ensure that lesion is in center of FOV in superior-inferior direction
Hints for oblique slab placement • Lower neck, chest, upper arms • Include descending thoracic aorta • Abdomen, upper pelvis • Include abdominal aorta • Lower pelvis • Include contra-lateral common iliac artery • Thigh • Include ipsi-lateral common femoral artery
Hints for oblique slab placement • Neck lesions • FOV to include upper and mid-descending thoracic aorta • Upper arm lesions • Image entire chest • In upper pelvis • FOV includes renal vessel origins • May need to check separate axial slices for correct slab placement including target lesion AND vessel • Use coronal localizer to confirm appropriate superior-inferior placement of oblique slab
Avoiding severe phase wrap artifact for DCE-MRI protocol 1) Patients who can tolerate the arms over head position should do so for the duration of the imaging. 2) If patients cannot tolerate this positioning, arms should be left at the side or lightly crossed over chest (avoiding kinking of IV line if placed in antecubital fossa). Arm positioning in these cases should be based on the following: a) if target lesion is posterior/lateral, place arms across chest (Figure a) b) if target lesion is anterior, place arms at side (Figure b) Figure a Figure b
Descending Aorta Target lesion Lung metastases
Aorta Target lesion Peri-aortic LN metastasis
Aorta Target lesion Gall bladder fossa metastasis (melanoma)
Aorta Target lesion Colon cancerMetastasis to peritoneum
Non-target lesion (too large, left lobe) Target lesion Aorta Colon cancerMetastasis to liver
T1 Mapping Series • Always during suspended end expiration • Slab prescription as described • Begin with flip angle = 30 degrees • Perform normal auto pre-scan procedure • Use 3 NEX for breath-hold (10-15 seconds) • Inspect for phase encode/wrap artifacts • Can increase FOV and rerun if required • Maintain new FOV for all subsequent oblique slab scans • Repeat above for flip angles 15, then 5 • Do NOT repeat automated pre-scan for flip 15 & 5 • Do NOT adjust receiver or transmitter gain
DCE-MRI Series – Set-up • Same slab prescription as T1 mapping • NEX < 1 (per phantom imaging) • Flip angle = 30 • Do NOT auto pre-scan between series • Acquisition for ~6 minutes (see chart next page) • Non breath-held • Instruct patient on quiet tidal respiration • Keep images in same series (if possible) • Can break into several series if needed • No delay between series once imaging begins
After installing parameters, the chart below will determine the number of scan phases/acquisitions/repetitions (see Form QC) • Set multiphase to total # of scan phases/acquisitions/repetitions • Set NO delay between phase acquisitions! • If machine error for multiphase imaging (as determined during phantom imaging) • Divide dynamic run into 2 series, ~3 min each • Each runs half the number of repetitions
DCE-MRI - Injection • Gadolinium contrast 0.1mg/kg • Injection rate 1.0 cc/sec • Saline flush, 20cc @ 1.0 cc/sec • Begin imaging pre gadolinium injection • Continue for 20-30 seconds before injection • Inject and continue scan ~6 minutes
Delayed post-gadolinium scans • Post gad T1 obl. cor. 2D fatsat FSPGR/FLASH • Oblique coronal, same thickness as DCE-MRI slab • No inter-slice spacing, interleaved acquisition • Same FOV and matrix as DCE-MRI slab • Prescribe at same location/obliquity/orientation • NEX=1, Breath-hold, end tidal expiration • Post gad T1 axial 2D fatsat FSPGR/FLASH • Same slice thickness/spacing as pre-gad T1 axial • Run through entire anatomic region • e.g. liver, lungs, pelvis • May run in several breath holds (end tidal exp.) as required
Cross-reference image of DCE-MRI • Choose axial image (T1, T2, post-gad) which demonstrates target lesion • Cross-reference obl. 3D slice locations • Remove annotations with patient identifiers! • Screen capture for submission to ACRIN Ax T2 image w/target lesion Same with cross referencing
Aorta Target lesion Colon cancerMetastasis to peritoneum
Kt = 0.11889 +/- 0.049131 Ve = 0.39289 +/- 0.14408 Kt = 0.1163 units [1/min] ve = 0.3870 units % Kt = 0.057848 +/- 0.013971 Ve = 0.35429 +/- 0.10141 Kt = 0.0575 units [1/min] ve = 0.3505 units % PRE POST
Target lesion Aorta Colon cancerMetastasis to liver
Kt = 0.31476 +/- 0.22599 Ve = 0.22779 +/- 0.10057 Kt = 0.3015 units [1/min] ve = 0.2070 units % Kt = 0.18454 +/- 0.15173 Ve = 0.16865 +/- 0.077324 Kt = 0.1235 units [1/min] ve = 0.1246 units % PRE POST
Site tumor/artery segmentation • Site PI must provide their own segmentation of tumor and artery from each DCE-MRI study • Choose portion of the dynamic gadolinium study that best demonstrates target lesion • (Often early gadolinium enhancement phase) • Use repetition with minimal motion artifact • Refer to pre-treatment study when segmenting post-treatment study • Attempt to include similar portions of tumor
Site tumor/artery segmentation • Identify all slices from DCE-MRI study which include portions of the target lesion • On local workstation, draw ROI (elliptical or freehand) to outline entire tumor • Include all tumor-bearing slice locations • Avoid major vessels or area of artifact • Repeat for maximally enhancing artery • Indicate segmentation slices on DP form • See example on next page
Name and DOB not visible Series, image number, & slice location visible Additional lesion (Ignore, do not segment) Target lesion Representative image from DCE-MRI study (early enhancement phase)
Exclude feeding vessels from ROI Different slice
Segmentation of Aorta In general, choose artery on central 2-4 slices within slab. Choose only maximally enhancing regions to avoid partial volume effects.
Complete DP form Questions 6-7 will capture site Radiologists analysis information TECHNOLOGIST RADIOLOGIST Page 1 Fax to 215-923-1737 Page 2
Indicate each slice location in 3D slab (OK to round to nearest mm) Check if tumor (or arterial) ROI is drawn on this slice Indicate series and image number used for segmenting Indicate area (in mm2) for each ROI Screen capture each slice/ROI combination to be sent to ACRIN. Indicate total # of screen captures here DP page 2 from previous example study: 12 slice DCE-MRI 11/12 slices with tumor ROI 3/12 slices with arterial ROI Tumor ROI Arterial ROI Leave later rows blank if 3D slab has fewer than 12 slices
Image Submission • Complete DP Form • Submit via email or fax • Transfer images via secure ftp • CD-ROM Shipment or TRIAD • Contact ACRIN at 215-940-8880 for more information regarding electronic image submission. Or contact Triad-Support@phila.acr.org • Include screen captures of the following: • Graphic Rx of Oblique scan cross-referenced on axial slice • Screen captures with tumor & arterial ROIs +
Remember • Choose optimal lesion for imaging • Patient positioning and comfort are key! • Breath-held T1 maps, then… • Instruct for quiet breathing during dynamic gadolinium DCE-MRI series • Replicate parameters and slab prescription on follow-up study • Have prior images available for review during follow-up DCE-MRI scanning session
Questions • Donna Hartfiel, data manager • dhartfiel@phila.acr.org • Jim Gimpel, chief technologist • jgimpel@phila.acr.org • Mark Rosen, principle investigator • rosenmar@uphs.upenn.edu