Download
1 / 16
260 likes | 538 Views
Sinusitis. Dr.Emamzadegan Ped.Cardiologist. Sinusitis. Sinusitis is a common illness of childhood and adolescence. Sinusitis. There are 2 types of acute sinusitis: viral bacterial. Sinusitis.

E N D
Sinusitis Dr.Emamzadegan Ped.Cardiologist
Sinusitis Sinusitis is a common illness of childhood and adolescence.
Sinusitis There are 2 types of acute sinusitis: viral bacterial
Sinusitis Approximately 0.5-2% of viral upper respiratory tract infections in children and adolescents are complicated by acute bacterial sinusitis.
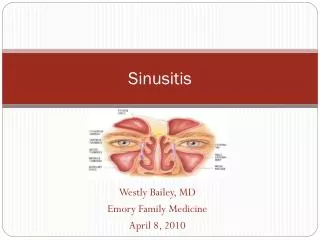
Sinusitis Both the ethmoidal and maxillary sinuses are present at birth, but only the ethmoidal sinuses are pneumatized . The maxillary sinuses are not pneumatized until 4 yr of age. The sphenoidal sinuses are present by 5 yr of age, whereas the frontal sinuses begin development at age 7-8 yr and are not completely developed until adolescence.
Ethiology The bacterial pathogens causing acute bacterial sinusitis in children and adolescents include Streptococcus pneumoniae (∼30%), nontypable Haemophilus influenzae (∼20%), and Moraxella catarrhalis (∼20%).
Ethiology Staphylococcus aureus, other streptococci, and anaerobes are uncommon causes of acute bacterial sinusitis in children. Although Staphylococcus aureus is an uncommon pathogen for acute sinusitis in children, the increasing prevalence of methicillin-resistant Staphylococcus aureus (MRSA) is a significant concern. H. influenzae,α- and β-hemolytic streptococci, M. catarrhalis, S. pneumoniae, and coagulase-negative staphylococci are commonly recovered from children with chronic sinus disease.
Clinical Manifestations Nasal congestion, purulent nasal discharge (unilateral or bilateral), fever, and cough. Less-common symptoms include bad breath (halitosis), a decreased sense of smell (hyposmia), and periorbital edema. Complaints of headache and facial pain are rare in children. Additional symptoms include maxillary tooth discomfort and pain or pressure exacerbated by bending forward. Physical examination might reveal erythema and swelling of the nasal mucosa with purulent nasal discharge. Sinus tenderness may be detectable in adolescents and adults. Transillumination reveals an opaque sinus that transmits light poorly.
Diagnosis The clinical diagnosis of acute bacterial sinusitis is based on history. Persistent symptoms of upper respiratory tract infection, including nasal discharge and cough, for >10-14 days without improvement, or severe respiratory symptoms, including temperature of at least (39 C) and purulent .nasal discharge for 3-4 consecutive days
Diagnosis of chronic sinusitis Children with chronic sinusitis have a history of persistent respiratory symptoms, including cough, nasal discharge, or nasal congestion, lasting >90 days.
Diagnosis • Sinus aspirate culture • Rigid nasal endoscopy • Findings on radiographic studies (sinus plain films, CT scans) including opacification, mucosal thickening, or presence of an air-fluid level are not totally diagnostic
Differential Diagnosis Differential diagnostic considerations include viral upper respiratory tract infection, allergic rhinitis, nonallergic rhinitis, and nasal foreign body.
Treatment It is unclear whether antimicrobial treatment of clinically diagnosed acute bacterial sinusitis offers any substantial .benefit
Treatment • Initial therapy with amoxicillin (45 mg/kg/day) • For the penicillin-allergic patient include trimethoprim-sulfamethoxazole, cefuroximeaxetil, clarithromycin, or azithromycin. • For children with risk factors (antibiotic treatment in the preceding 1-3 mo, daycare attendance, or age <2 yr) for the presence of resistant bacterial species, and for children who fail to respond to initial therapy with amoxicillin within 72 hr, treatment with high-dose amoxicillin-clavulanate (80-90 mg/kg/day of amoxicillin) should be initiated.
Treatment Treatment is recommended for 7 days after .resolution of symptoms
Complications • periorbitalcellulitis and orbital cellulitis • epidural abscess • Meningitis • cavernous sinus thrombosis, • subdural empyema, • brain abscess • osteomyelitis of the frontal bone (Pott puffy tumor), • mucoceles