Download
1 / 34

E N D
Basic ATLS ThePrimarySurvey JasonSmithMDDMIFRCS(Gen.Surg) ConsultantSurgeon
Trauma - expression comprising a spectrum of severity of mechanical violation of tissues, from a little scratch to a multiply injured patient. - also surgical intervention.
Dying fromTrauma Jason Smith, Consultant Surgeon
An organized consistent approach to the trauma patient optimal outcome. The Advanced Trauma Life Support (ATLS) developed in 1976, adopted by the American College of Surgeons in 1979, and the UK in1989 The primary focus of ATLS is on the first hour of trauma management - rapid assessment and resuscitation THE GOLDEN HOUR
Trauma Mxinvolves: 1.Preparation 2.Triage 3.PrimarySurvey(ABCDEs) 4.Resuscitation 5.Adjunctstoprimarysurvey&resuscitation 6.SecondarySurvey(headtotoeevaluation&history) 7.Adjunctstosecondarysurvey 8.Continuedpost-‐resuscitationmonitoring&re-‐evaluation 9.DeTinitecare. ! ! ! ! ! ! ! ! ! Jason Smith, Consultant7Surgeon 1/00
Initial Assessment/Management Primary Survey Iden%fiesmostlife-‐threateninginjuries ! Resuscita0on Airwaycontrol Ensure oxygena0on / ven0la0on Needle / tubethoracostomy ! ! ! Jason Smith, Consultant Surgeon
1/00 10
Primary survey-‐immediatelife-‐threats Jason Smith, Consultant Surgeon
Adjuncts andtests Adjuncts Pulseoximeter Cardiacmonitor Foleycatheter NG tube Diagnos%ctests CXR Pelvicx-‐ray C-‐spinex-‐ray • ! ! • • • • • • • ECG • Pregnancytest • Bloods Jason Smith, Consultant Surgeon
PRIMARY SURVEY 13 1/00 Jason Smith, Consultant Surgeon
PRIMARY SURVEY PrioritiesforthecareofAdult, Paediatric& Pregnantwomenareall same! the During threatening the primary survey life conditionsareidentified and management is instituted SIMULTANEOUSLY. Jason Smith, Consultant Surgeon
A.AirwayMaintenancewithCervicalSpineControl GCSscoreof8orlessrequiretheplacementof definite airway. Protec%onofthespine&spinalcordistheimportant managementprinciple. Neurological examalonedoesnotexcludeacervical spine injury. Alwaysassumeacervicalspineinjuryinanyptwithmul%-‐systemtrauma,especiallywithanalteredlevelofconsciousnessorbluntinjuryabovetheclavicle. ! ! ! ! Jason Smith, Consultant Surgeon
A–HowTo? ChinLiPorJawthrust?? Inspectairway? Maintainorassist? Op%ons: ! ! ! ! ! Simply openit! Deliver O2–asmuchaspossible? BagValvemask? Guedel /Nasopharyngeal? Laryngealmask? Endo/NasoTrachealtube? Surgical Airway ! ! ! ! ! ! Andyoudon’tforget??????? ! Jason Smith, Consultant Surgeon
Airway withCervicalSpineControl Jason Smith, Consultant Surgeon
B.Breathing & Ventilation Airwaypatencydoesnotassureadequateven%la%on. ! orrebreather Bag/Valvemask HighflowO2 ! ! 20 1/00 Jason Smith, Consultant Surgeon
B–Howto? Needanadequateairway ProvidehighflowO2 Decompresstensionpneumo Thoracostomy? ChestDrain FlailChest? ! ! ! ! ! ! Jason Smith, Consultant Surgeon
Life-‐threateningChestTrauma Primary Survey Airwayobstruc0on Tensionpneumothorax Openpneumothorax Flailchest Massivehaemothorax Cardiactamponade ! ! ! ! ! ! Jason Smith, Consultant Surgeon
Breathing TensionPneumothorax: Signs / Symptoms Respiratorydistress Distendedneckveins Unilateral in breath sounds Hyper-‐resonance Cyanosis, late ! ! ! ! ! Jason Smith, Consultant Surgeon
Breathing OpenPneumothorax Coverdefect Chesttube Defini%veopera%on ! ! ! Jason Smith, Consultant Surgeon
Breathing Flail Chest Jason Smith, Consultant Surgeon
C.CirculationwithHaemorrhageControl. a.consciousness. b. skincolor c.Pulse. externalbleedingisiden%fied& controlledintheprimarysurvey. Tourniquetsshouldnotbeused** ! ! ! ! ! Jason Smith, Consultant Surgeon
C–Howto? Adequateairway AdequateVen%lla%on 2largeborevenflons(PoiseuilleLaw) 2litrescrystalloid Controlbleedingpoints Resuscita%velaparotomy Resuscita%vethoracotomy ! ! ! ! ! ! ! F α 1/l and F αd Jason Smith, Consultant Surgeon
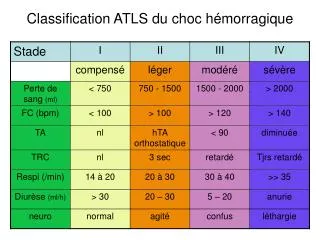
Fluid&BloodLoss ClassI ClassII ClassIII ClassIV BldLoss(mls) 750 750-1500 1500-2000 >2000 BldLoss(%vol)15% 15-30% 30-40% >40% HR <100 >100 >120 >140 BP N N ↓ ↓ PP Nor↑ ↓ ↓ ↓ RR 14-20 20-30 30-40 >35 UO >30 20-30 5-15 -- CNS SlightlyMildlyanxiousAnxious& Confused& anxiousconfused lethargic FluidreplacementCrystalloidCrystalloidCrystalloid& Crystalloid& blood blood OUTCOME✔✔✓/✖✖ Jason Smith, Consultant Surgeon
Circulation–LifeThreateningConditions MassiveHaemothorax CardiacTamponade Anymajorvessel Anymajorbone Anysolidorgan Pregnantwomen ! ! ! ! ! ! Jason Smith, Consultant Surgeon
D.Disability(NeurologicalEvaluation) Simple Mnemonictodescribelevelofconsciousness A:Alert V:RespondstoVocals%muli P:RespondstoPainfuls%muli U:Unresponsivetoalls%muli ! ! ! ! ! NotforgettousealsoGlascowComaScale (secondary Survey). ! Jason Smith, Consultant Surgeon
E.Exposure/EnvironmentalControl Itisthept’sbodytempthatismostimportant,not the comfortofthehealthcareprovider. Intravenousfluidshouldbewarm. Warm environment(roomtem)shouldbe maintained. early controlofhemorrhage. ! ! ! ! Jason Smith, Consultant Surgeon