Download
1 / 24
250 likes | 257 Views
Antihypertensive Agents. Dr S. O. Olayemi. HYPERTENSION. Chronically persistent elevated blood pressure>/=140 mm Hg systolic blood pressure and or diastolic >/= 90 mmHg in individual above 18 years of age Controlled BP SBP <140mmHg and DBP<90mmHG. Expert Committee on non Communicable diseases.

E N D
Antihypertensive Agents Dr S. O. Olayemi
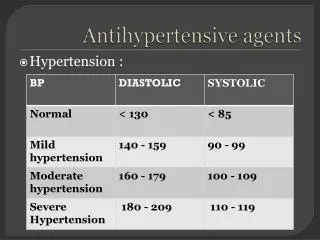
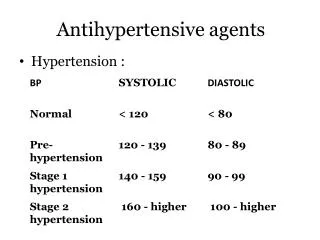
HYPERTENSION Chronically persistent elevated blood pressure>/=140 mm Hg systolic blood pressure and or diastolic >/= 90 mmHg in individual above 18 years of age Controlled BP SBP <140mmHg and DBP<90mmHG
Expert Committee on non Communicable diseases • One third of Nigerian adults above 15 years of age are hypertensives, from this one third are aware of the hypertensive status, and one third are on treatment. • Control definition?Complex?compliance/cost etc
TREATMENT GOAL Prevent morbidity and mortality associated with high blood pressure. Achieving control through least intrusive means possible Control other modifiable cardiovascular risk factors.
Ace Inhibitors: • Captopril (Capoten) 12.5 – 150mg daily • Enalapril (Vasotec) 5 – 40 mg daily • Lisinopril (Zestril) 5 – 40mg daily • Ramipril (Tritace) 2.5 – 10mg daily • Perindopril (Aceon) 4 – 16 mg daily • Fosinopril (Monopril) 5 – 40mg daily
Action: ACEI block conversion of Angiotensin 1 to Angiotensin 11 thereby blocking stimulation of aldosterone. • Major site of Angiotensin II production – Vessels and not the kidneys. • reduce peripheral resistance and salt and water retention. • Side Effect: Cough, Rashes, Leukopenia, Hyperkalaemia, Angio-Odema
ACE inhibitors • Reduce dose in volume depleted pt, elderly(hypotension) • May be combined with diuretics • Hyperkalaemia – CKD pts, potassium sparing diuretics and angiotensin receptor blockers. • ARF- renal artery stenosis • Contraindicated in pregnancy and pt with hx of angioodema.
ANGIOTENSIN II RECEPTOR ANTAGONISTS • Losartan (Cozaar) 50 – 100 mg daily • Valsartan (Diovan) 80 – 320 mg daily • Temilsartan (Micardis) 20 – 80 mg daily • Irbesartan (Avapro) 150 –300mg daily • Olmesartan (Benicar) 20 – 40 mg daily • Candesartan (Atacand) 8 – 32 mg daily
ANGIOTENSIN II RECEPTOR ANTAGONISTS: ARBs • Action: They directly block the angiotensin II type 1 (AT1) receptors – vasoconstriction, aldosterone release, sympathetic activation, ADH release, constriction of efferent renal arterioles • Beneficial AT2-vasodilation,tissue repair and inhibition of cellular growth in blood vessels (reduce peripheral resistance and salt/water retention) • Side Effects: Rashes, Leukopenia,Hyperkalaemia but no cough
ARBs • Reduce dose in volume depleted pt, elderly(hypotension) • May be combined with diuretics • Hyperkalaemia – CKD pts, potassium sparing diuretics and angiotensin receptor blockers. • ARF- renal artery stenosis • Contraindicated in pregnancy • Do not induce cough as in ACEIs
VASODILATORS ; Hydralazine (Apresoline 20 – 100 mg daily, Minoxidil (Loniten) 10 – 40mg daily, • Action: They decrease peripheral resistance by dilating arteries/arterioles. • Combined with diuretic/B blockers –diminish fluid retention/reflex tarchycardia. • Side Effect: Hydralazine (Headache, lupus-like syndrome), • Minoxidil (Orthostasis, facial hirsutism), • Diazoxide (Hyperglycaemia.
CALCIUM CHANNEL BLOCKERS • Dihydropyridines : • Nifedipine (Adalat/ProcardiA) 20 – 90 mg dly, I, Felodipine (Plendil) 5 – 20 mg dly, • Amlodipine (Norvasc) 2.5 – 10 mg dly • Nicardipine (Cardene) 60 – 120 mg dly • Phenylakylamine: Verapamil 100 – 400 mg dly • Benzothiazepine: Diltiazem 120 – 480 mg dly. • Action: Reduce smooth muscle tone and cause vasodilation: may reduce cardiac output. • Verapamil/diltiazem: decrease HR/delay A-V nodal conduction – Supra ventricular tachycardia
Calcium channel blockers • Avoid immediate release nifedipines etc • Dihydropyridines are more potent peripheral vasodilators compared to non-dihydropyridines. • Side effect: Dihydropyridines – reflex sympathetic discharge (tarchycardia) Headache, flushing, peripheral oedema. • Non dihyropyridines – variable heart block
DIURETICS • Loop diuretics – Frusemide (Lasix) 20mg – 1 g, Bumetanide (Bumex) 0.5-4mg Torsemide (Demadex) – 5mg dly. • Site of Action: Loop of Henle, Reduce Na+/K+/Cl- cotransporter: reduce urine concentration; Increase calcium excretion. • Preferrably morning/afternoon (avoid nocturnal diuresis) • Higher doses in patients with CKD. • Side effect: Ototoxicity, Hypokalaemia, Hypotension, Gout.
DIURETICS: • Thiazides: Chlorthalidone (Hygroton) 6.25 – 25mg dly, Hydrochlorothiazides (Esidrix) 12.5 – 50mg dly Bendrofluazide 2.5 – 5mg dly • Site of Action: Early distal tubule, they reduce NaCl reabsorption thereby reducing the diluting capacity of nephron. Decrease Calcium excretion. • Dose in Morning (avoid noctunal diuresis) • More effective antihypertensives than loops except in CKD (GFR <30ml/min • Side effects: Hypokalaemia, Hyponatreamia, Hypercalcemia, Hyperglyceamia, Hyperlipidaemia, Hyperuricaemia (Problematic in gout),
Potassium sparing diuretics • Aldosterone antagonist: Spironolactone (Aldactone) 25 –50 mg dly, Epleronone (Inspra) 50 – 100 mg dly • Site of Action: Cortical collecting tubule, They block Na+ channels • Side effects: Hyperkalemia, Sexual dysfunction • Potassium Sparing: Amiloride/hydrothiaz-Moduretic 5 – 10/50 –100 mg dly, • Triamterene/hydrothiaz 37.5 – 75/25 50 mg dly • Aldosterone antagonist : Gynaecomastia. • Action: Reduce extracellular fluid volume and thereby reduce vascular resistance
CENTRALLY ACTING DRUGS: Methyl dopa (Aldomet) 250mg – 1g dly, Clonidine (Catapres) 0.1-0.8mg dly, • Action:They inhibit Sympathetic Nervous System via Central Alpha 2 Adrenergic Receptors. • Clonidine withdrawal –Rebound BP elevation • Side Effects : Somnolence, Orthostasis, Impotence, Rebound Hypertension • RESERPINE (0.05-0.25mg) dly- • Combined with diuretics-reduce fluid retention
BETA BLOCKERS • Selective Cardioselective: Atenolol (Tenormin) 25 – 100 mg dly, Metropolol (Lopressor) 50 – 200mg dly, Bisprolol (Zebetal) 2.5-10mg dly Bexalolol (Kerlone) 5-20 mg dly. • Non Selective: Propranolol (Inderal) 40-320mg dly, Nadolol(Corgard) 40 – 120mg dly, Timolol Blocaden) 10 – 40 mg dly. • Intrinsic Sympathomimetic activity: Pindolol (Visken) 10 – 60mg dly, Penbutolol(Levatol) 10 – 40mg dly, Acebutolol (Sectral) 200 – 800 mg dly. • Alpha and Beta Blockers: Labetalol (Trandate • 200-800 mg dly, Carvedilol (Coreg) 12.5 –50mg dly).
Beta Blockers • Actions: They reduce cardiac contractility and Rennin release. • Additional benefit-Tarchyarrythmias,essential tremor, migraine headache and thyrotoxicosis • Side Effect: Bronchospasm ( in severe asthma), bradycardia (A-V Block), Congestive Heart Failure exacerbation, impotence, fatigue, depression. • Abrupt withdrawal-rebound hypertension.
Antihypertensive Medications indicated in specific Patient Population • Diabetes with proteinuria • Ace Inhibitors (ACEI) • Congestive Heart Failure ACEI, Diuretics +/-Beta Blockers • Isolated systolic Hypertension • Diuretics preferred: long acting dihyropyridine calcium channel blockers
CONTD • MI Beta Blockers without intrinsic sympathomimetic activity, ACEI • Osteoporosis Thiazide diuretics • BPH Alpha antagonists • Pregnancy Methyldopa, Beta blockers, Labetalol, Hydralazine +/-calcium antagonists
Antihypertensives in pregnancy • Methyldopa-preferred based on safety data • B Blockers- Safe, but IUGR reported • Labetalol-preffered over methyldopa because of fewer side effects • Clonidine- Limited data available • CCBs-Limited data available, no teratogenicity with exposure • Diuretics-not first line agents but probably safe in low doses • ACEIs/ARBs- major teratogenicity on exposure
JNC 7 MANAGEMENT OF HYPERTENSION • Prehypertension 120-139/80-89- Life style modification. • Stage 1 140-159/90-99-Thiazides, may consider ACEI,ARB, B Blockers Calcium blockers or a combination • Stage 2 >160/>100 – Two drug combination (usually a thiazide diuretic+an ACEI, an ARB, a B blocker, or calcium blocker
THE END • THANK YOU.